


As an optometrist in an integrated ophthalmology and optometry practice, I treat many patients who are considering refractive surgery or recovering from a procedure. Our practice recently added the minimally invasive, small incision lenticule extraction (ReLEx SMILE; ZEISS) for patients who are myopic with a refraction of -1.00 D to -8.00 D with 0.50 D or less of astigmatism. The first minimally invasive, single-laser refractive option, the SMILE procedure has been proven safe and effective and has been used in more than a million cases.1,2 I am very excited about the unique characteristic of this procedure, and so are my patients.
A Minimally Invasive Option
We have long had a very good refractive surgery platform and “gold standard” procedures, but we are not complacent. We want to keep growing and improving, giving patients more and more options to best fit their needs and goals. Like any ophthalmic surgery, refractive procedures are part of the decades-long evolution toward preserving corneal anatomy—an evolution that depends on continual innovation.
I have had the privilege to work with many patients who have glaucoma, including many who have had microinvasive glaucoma surgeries (MIGS). MIGS technologies have been a revolutionary change for glaucoma patients, who now have new, less invasive options to meet their needs. I think of the SMILE procedure as another tool in our toolbox to help meet the needs of our patients. If everyone got complacent and just continued to follow the norm, we would not have the advances in MIGS or in the SMILE procedure.
In the SMILE procedure, the surgeon reshapes the cornea by making a lenticule in the corneal stroma using the VisuMax laser (ZEISS) and removing it through a small incision at 60° to 90°. With no flap and a smaller side-cut than LASIK, the SMILE procedure reduces cutting and damage to the corneal tissue.3
Corneal innervation enables the eye to tell the brain it is dry and prompt tear production—a key part of keeping the eye well hydrated. When there is less corneal nerve damage in the process of refractive surgery, I expect to see less dryness and maybe less fluctuation in vision long term when compared to LASIK.3 This is potentially better for all eyes, but it particularly benefits patients who we are concerned may have dry eye after refractive surgery.
In addition, the corneal biomechanics of the SMILE procedure have been compared to other refractive surgery platforms recently. Researchers found that because the SMILE procedure disrupts the anterior stroma less than LASIK, it produces less corneal biomechanical change, which in turn enables the cornea to maintain its anatomic state.4
Finally, the SMILE procedure is performed entirely with a femtosecond laser, rather than both the femtosecond and excimer laser used for LASIK. I think new surgeons just starting out in refractive surgery may prefer this approach.
Educating Patients and Referring ODs
I frequently talk to patients who are unhappy in glasses or contact lenses about the refractive procedures available to them. I have deep, vested, long-term relationships with my patients built on trust, and my counseling helps them make better-informed decisions.
I explain to my SMILE patients that the procedure is very short and very safe.1,2 I talk through how the procedure works and we discuss postoperative expectations. I expect their vision to be better on day 1 than it was before surgery, but their best vision will be reached about 3 to 4 weeks later. They may have some dryness after having any refractive procedure, although the SMILE procedure causes less dryness than some other procedures, and there may be visual fluctuations during healing. I also explain how the healing process is likely to look over the following weeks and months.
During our practice’s adoption of the SMILE procedure, my colleagues and I have been very proactive about educating referring optometrists. Our practice is built on optometric referrals. About 90% to 95% of the patients that come through our door are referred from a primary optometrist. We work very hard to maintain good relationships with our optometrists through education and management.
With SMILE, we set up symposia, webinars, and evening meetings to give referring optometrists convenient opportunities to get an in-depth look at SMILE. In addition to making good business sense, this process—with SMILE and other technologies—has been enjoyable. As a community, we all share the same enthusiasm for helping our patients achieve clear vision and healthy eyes, which makes this new refractive surgery an exciting advance.
Case Study
The patient: As one of the sub investigators in the FDA clinical trial for the SMILE procedure, I got to comanage this procedure for a very dear friend of mine.1 The patient is a 28-year-old social worker who loves yoga and reading and was tired of wearing glasses and contact lenses.
Current vision correction: OD: -2.50-0.25×11, OS: -3.00-0.50×22
Preoperative measurements: The patient had minimal higher-order aberrations and smooth topography. She did not have thin corneas.
SMILE candidacy: The patient’s refraction was within range for the SMILE procedure (-1.00 D and -8.00 D with astigmatism of 0.50 D or less) (Figure 1). Corneal topography made her a good candidate for SMILE as well (Figure 2). She had mild dry eye that reduced her contact lens wear time.
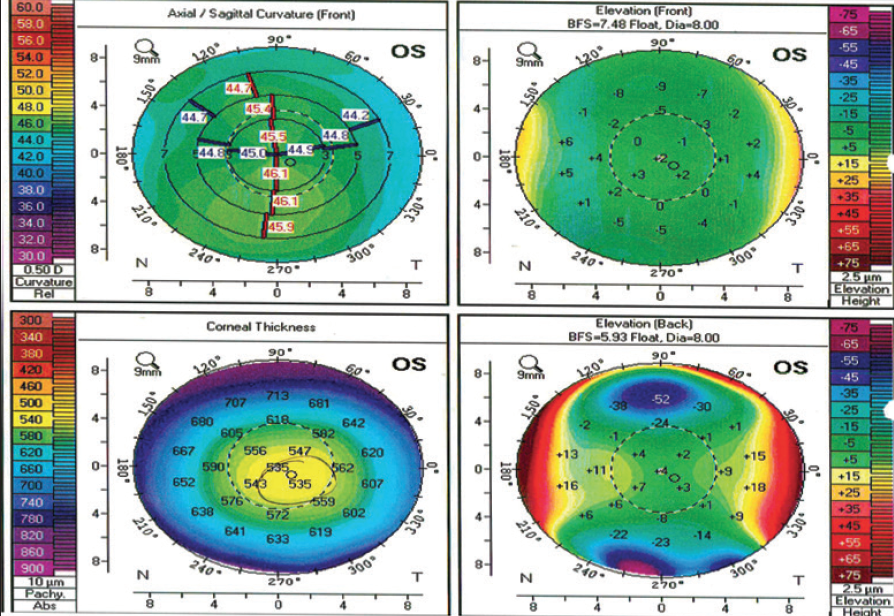
Figure 1. Pentacam (Oculus) shows good corneal symmetry on front axial map, no concerning posterior float changes, and average corneal pachymetry.
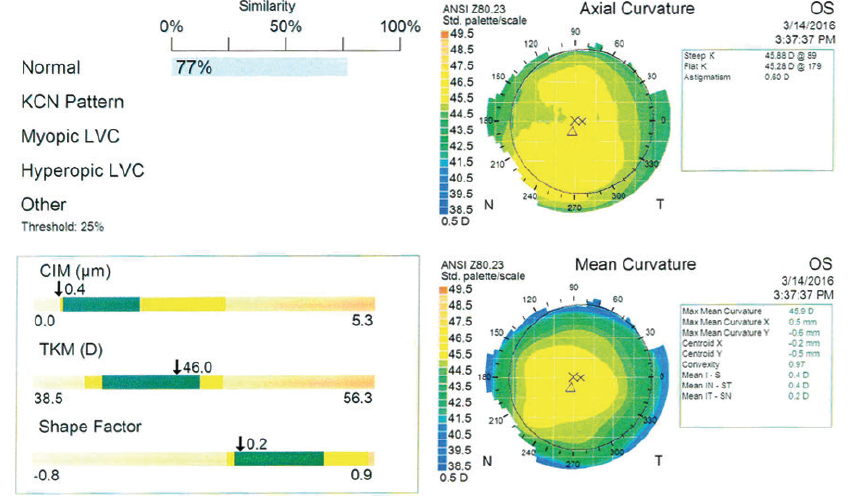
Figure 2. Atlas 9000 (ZEISS) corneal topography shows average to steep Ks and low corneal astigmatism.
Procedure: Because the patient was enrolled in the FDA clinical trial, which required LASIK in one eye and SMILE in the fellow eye, she had SMILE on her left eye and LASIK on the right. (Typically, if a patient is a candidate for SMILE, both eyes can receive the procedure.) Using a femtosecond laser (VisuMax; ZEISS), the surgeon made a lenticule in the left eye and removed it to reshape the cornea. A CustomVue (Visx) scan of the right eye showed low amounts of corneal higher-order aberrations with coma and trefoil, which helped us decide the patient should have wavefront-guided LASIK. After surgery, the patient used prednisolone acetate (Pred Forte; Allergan) 4 times a day for 1 week tapering to 2 times per day for 3 weeks and moxifloxacin (Vigamox; Novartis) 4 times a day for 1 week.
Outcome: My friend is very happy with the outcome of surgery. She says that waking up in the middle of the night without needing to find her glasses or put in contacts has been a breath of fresh air. Her Snellen uncorrected vision on her 1-day postoperative check was 2 lines superior in her LASIK eye compared to the SMILE eye. I explained that the SMILE eye was going to take just a little bit longer to reach clear, crisp vision. Four weeks later, she was 20/15 uncorrected in both eyes. She is doing great and enjoying her new life without wearing glasses and contacts.
- Data on file. Carl Zeiss Meditec, Inc.
- Blum M, Täubig K, Gruhn C, et al. Five-year results of small incision lenticule extraction (ReLEx SMILE). BJO. 2016.100;9:1192.
- Denoyer A, Landman E, Trinh L, et al. Dry eye disease after refractive surgery: comparative outcomes of small incision lenticule extraction versus LASIK. Ophthalmology. 2015;122(4):669-676.
- Reinstein DZ, Archer TJ, Randleman JB. Mathematical model to compare the relative tensile strength of the cornea after PRK, LASIK, and small incision lenticule extraction. J Refract Surg. 2013;29(7):454-460.