

Glaucoma is a complex disease to diagnose and manage. It’s all about controlling risk factors and monitoring progression over time. Traditionally, topical drops have been the go-to for first-line therapy, and although modern medications work well, they rely on patient adherence. One thing I’ve learned over the years regarding adherence is that patients with glaucoma often stretch the truth about how well they stick to their drop regimen.
AT A GLANCE
- Minimally invasive glaucoma surgery (MIGS) is a term used for safe, convenient, and effective procedures that enable earlier intervention of the disease process, allowing treatment to be proactive rather than reactive.
- MIGS procedures fall into two categories: those that increase outflow and those that decrease aqueous production; major differences depend on the targeted anatomy.
- The advantage of MIGS procedures is that oftentimes, several of them can be combined to create compounding effects.
- With the new tools available that have proven safe and efficacious, procedural treatments can and should be considered earlier to prevent permanent vision-altering progression.
Minimally invasive glaucoma surgery (MIGS) is an umbrella term used to describe procedures that have become popular in the management of glaucoma. These procedures are safe, convenient, and most importantly, effective. They allow us to intervene earlier in the disease process with less risk, which means we can be proactive rather than reactive—and that is the true essence of interventional glaucoma. Several surgical procedures are available to treat glaucoma. Each has different advantages and disadvantages. We go into more depth here.
MORE ON MIGS
MIGS procedures fall into two categories: those that increase outflow and those that decrease aqueous production. Major differences depend on the targeted anatomy, specifically the trabecular meshwork/Schlemm canal, suprachoroidal space/subconjunctival space, and ciliary body. The advantage of MIGS procedures is that often, we can combine several of them to create compounding effects.
MIGS Procedures That Increase Outflow
When explaining MIGS procedures to our patients, we use the analogy of a bathtub with a faucet that’s constantly running and a drain plug letting out excess water. What happens if the drain becomes plugged? Water ends up all over the floor. We need to unplug the drain. Stents, goniotomies, viscocanaloplasties, and subconjunctival stents all increase outflow.
The first MIGS glaucoma trabecular meshwork bypass stent received FDA approval in 2012. It was a single device made of titanium that was implanted into Schlemm canal during cataract surgery. It had the appearance of a snorkel, with the short end sticking into the anterior chamber. Providing only a modest improvement, it was phased out after a two-stent system gained FDA approval in 2018. These stents are performed in combination with cataract surgery. A more recent, three-stent system has been approved for use as a standalone procedure in patients who have failed with medications or those with previous glaucoma surgery. The autoinjector comes equipped with three stents, each designed to be placed roughly 2 clock hours apart in the nasal angle. In its pivotal trial, 73.4% of participants achieved a decrease in IOP of 20% or more, while 47.4% of participants achieved a decrease in IOP of 30% or more.1 These stents carry a high safety profile and, due to the system’s relative ease of use intraoperatively, it has grown in favor with both cataract and glaucoma surgeons alike.
As with the trabecular meshwork bypass stents, the Schlemm canal microstent is designed to increase outflow via Schlemm canal. The 8-mm stent spans 90˚ of Schlemm canal, acting as a scaffold. In pivotal trials, it showed results comparable with the 3-stent trabecular meshwork bypass stent, with 77.3% achieving a reduction in IOP of 20% or more.2
Rather than implanting a device, another option is removing tissue, as is performed with a goniotomy. These devices display great IOP control postoperatively.3 A dual-blade goniotomy device is a single-use disposable device with a ramp and parallel 230-µm blades. Think of it as a shovel that removes trabecular meshwork, exposing collector channels of Schlemm canal. In pivotal trials, 57.7% of participants experienced an IOP reduction of more than 20% at 1 year.4 Medications decreased from 1.6 to 0.8 in that time period.4
Viscocanaloplasty plus trabeculotomy is a twist on goniotomy, except it combines a trabeculotomy with canaloplasty. This is essentially a two-step procedure. First, a catheter is inserted into the nasal trabecular meshwork to access Schlemm canal. The catheter is extended 180°, and upon retraction, cohesive viscoelastic is injected. The procedure can be repeated on the other 180° of Schlemm canal for a full 360° of treatment. Then, similar to the procedure performed with goniotomies, Schlemm canal is unroofed through a “ripcord” maneuver using the catheter. The GEMINI trial showed that 77% of participants achieved more than a 20% reduction in IOP after 24 months.5
Subconjunctival stents target a different anatomic area—the subconjunctival space. They create a “mini bleb” and consequently walk the line of “minimally invasive” glaucoma procedures, as the process is similar to its more invasive cousin, the traditional trabeculectomy. Subconjunctival stents bypass the trabecular meshwork to the subconjunctival space and are considered easier to perform than a trabeculectomy by most. The procedure is for more moderate to advanced glaucoma, as it is approved for refractory glaucoma. Antimetabolites such as mitomycin C are often used to prevent bleb scarring; however, the bleb can be problematic and require attention to ensure it’s functioning properly. Still, according to recent studies, 76.5% of patients achieved a primary endpoint of greater than 20% IOP reduction.6
MIGS Procedures That Decrease Aqueous Production
Another strategy we can employ is suppressing aqueous production through cyclodestruction, which is the process of downregulating the production of aqueous by destroying processes of the ciliary body. Endocyclophotocoagulation (ECP) is a technique that uses a laser diode to blanch or contract individual ciliary processes. This can be done using a video monitor endoscopically 180° to 360° around the ciliary body. Transscleral cytophotocoagulation is similar to ECP in that the target is individual ciliary processes. Contrary to ECP, with transscleral cytophotocoagulation, a diode is placed on the limbus and energy is transmitted transclerally, as the name implies. The advantage of ECP is that it allows a more targeted treatment to individual ciliary processes, minimizing collateral damage to neighboring structures.7
ON THE HORIZON
Laser trabeculostomy is a new idea that uses lasers to directly treat the trabecular meshwork and increase outflow. Two types of lasers are showing promise: excimer laser trabeculostomy (ELT) and femtosecond laser, image-guided, high-precision trabeculotomy (FLigHT).8 Contrary to the more familiar selective laser trabeculectomy (see A New Twist on an Old Procedure), which relies on alteration of biochemical properties of the trabecular meshwork, ELT/FLigHT create channels that allow direct access to Schlemm canal (Figure 1).

Figure 1. Day 1 gonioscopic image of an image-guided femtosecond laser channel allowing direct access to Schlemm canal.
In ELT, holes are created through the trabecular meshwork via an ab interno approach. FLigHT, on the other hand, does not require incisions. Using a high-resolution gonioscopic image, the trabecular meshwork can be treated through the cornea (Figure 2). The first in-human trial of FLigHT showed promising results after 2 years, with a mean IOP reduction of 34.6% and 82.3% of participants achieving more than a 20% IOP reduction compared with baseline.9 This technology is similar in theory to the trabecular meshwork bypass stents. With it, we are creating a channel to directly access Schlemm canal. Although the trabecular meshwork bypass stents are implanted at different clock hours, there may be application for more aggressive treatment with ELT/FLigHT creating additional channels around the clock.
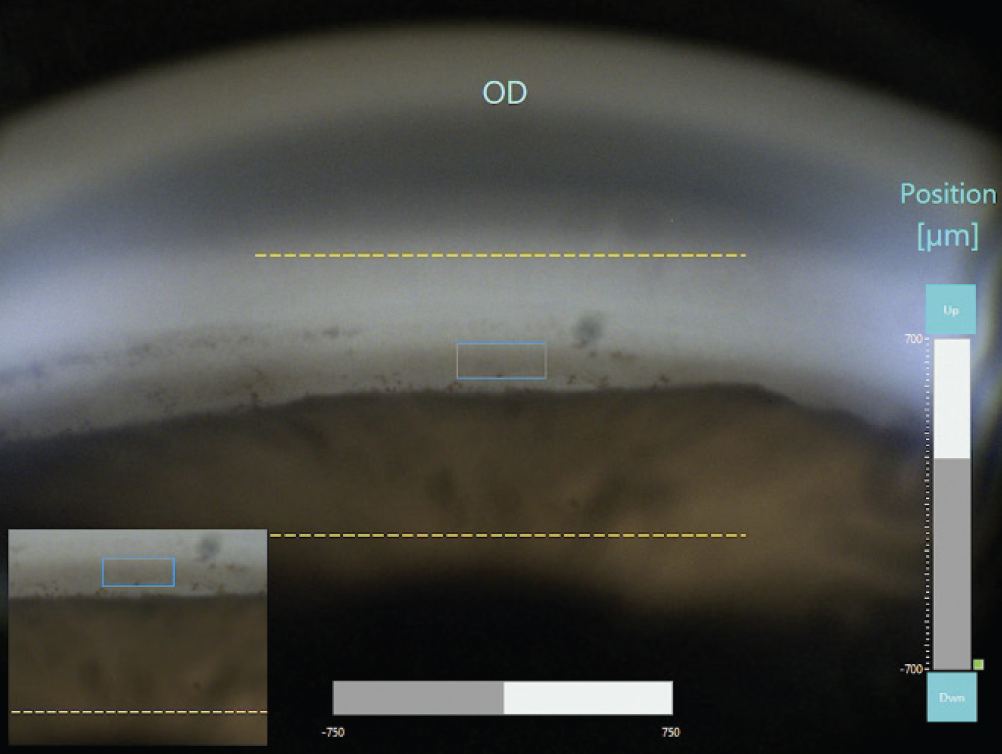
Figure 2. Using a femtosecond laser, we can accurately target the trabecular meshwork and allow access to Schlemm canal as seen here.
A New Twist on an Old Procedure
Selective laser trabeculectomy (SLT) has been around for more than 2 decades, and its cousin, argon laser trabeculoplasty, has been around since the 1970s. Thanks to the LiGHT trial, SLT has a more prominent place in our repertoire as a first-line therapy.1 Direct SLT was FDA-approved in December 2023. Traditional SLT applies low-energy Nd:YAG directly to the trabecular meshwork using a gonio lens. It is cost-effective and efficacious, providing substantial IOP-lowering power in a noninvasive manner. Visualization of the trabecular meshwork using a gonio lens can be tricky; a certain level of skill and experience is needed. Direct SLT provides an automated method that is non-contact and translimbal (ie, no gonio lens required). It provides the benefit of a quicker procedure and less variability induced by doctor experience and skill level.
1. Gazzard G, Konstantakopoulou E, Garway-Heath D, et al; LiGHT Trial Study Group. Laser in Glaucoma and Ocular Hypertension (LiGHT) Trial: six-year results of primary selective laser trabeculoplasty versus eye drops for the treatment of glaucoma and ocular hypertension. Ophthalmology. 2023;130(2):139-151.
CHANGING THE PARADIGM
The concept of interventional glaucoma is becoming more widely accepted. In decades past, treatment meant taking a conservative approach (ie, topical drops), waiting for true signs of progression, and reserving surgery as a last resort. With the new additions in our toolbox that have proven safe and efficacious, procedural treatments can and should be considered earlier to prevent permanent vision-altering progression.
1. Sarkisian SR Jr, Grover DS, Gallardo MJ, et al; iStent infinite Study Group. Effectiveness and safety of iStent Infinite Trabecular Micro-Bypass for uncontrolled glaucoma. J Glaucoma. 2023;32(1):9-18.
2. Ahmed IIK, De Francesco T, Rhee D, et al; HORIZON Investigators. Long-term outcomes from the HORIZON randomized trial for a Schlemm’s canal microstent in combination cataract and glaucoma surgery. Ophthalmology. 2022;129(7):742-751.
3. Vasu P, Abubaker Y, Boopathiraj N, et al. Clinical outcomes of excisional goniotomy with the Kahook dual blade: 6-year results. Ophthal Ther. 202413(10):2731-2744.
4. Dorairaj S, Radcliffe NM, Grover DS, Brubaker JW, Williamson BK. A review of excisional goniotomy performed with the Kahook dual blade for glaucoma management. J Curr Glaucoma Pract. 2022;16(1):59-64.
5. Greenwood MD, Yadgarov A, Flowers BE, Sarkisian SR Jr, Ohene-Nyako A, Dickerson JE Jr; GEMINI 2 Study Group. 36-month outcomes from the prospective GEMINI study: canaloplasty and trabeculotomy combined with cataract surgery for patients with primary open-angle glaucoma. Clin Ophthalmol. 2023;17:3817-3824.
6. Grover DS, Flynn WJ, Bashford KP, et al. Performance and safety of a new ab interno gelatin stent in refractory glaucoma at 12 months. Am J Ophthalmol. 2017;183:25-36.
7. Pantcheva MB, Kahook MK, Schuman JS, Noecker RJ. Comparison of acute structural and histopathological changes in human autopsy eyes after endoscopic cyclophotocoagulation and trans-scleral cyclophotocoagulation. Br J Ophthalmol. 2007;91:248-252.
8. ViaLase receives CE mark for first femtosecond laser for the treatment of glaucoma, the ViaLase Laser | ViaLase [press release]. ViaLase. July 30, 2024. Accessed December 12, 2024. www.vialase.com/vialase-receives-ce-mark-for-first-femtosecond-laser-for-the-treatment-of-glaucoma-the-vialase-laser/
9. Nagy ZZ, Kranitz K, Ahmed II, De Francesco T, Mikula E, Juhasz T. First-in-human safety study of femtosecond laser image-guided trabeculotomy for glaucoma treatment: 24-month outcomes. Ophthalmology Science. 2023;3(4):100313.



