

Nearly 1.7 million brain injuries occur in the United States each year.1 More than half of the brain’s cortex is dedicated to processing visual information.2 Blurry vision, difficulty reading, light sensitivity, double vision, and visual field defects are among the ocular symptoms that can be associated with brain injuries. Concussion is the most common type of brain injury, and impaired eye tracking is a symptom of postconcussion syndrome, which can occur immediately after the initial trauma and last years after.3
Optometrists are perfectly positioned to analyze and treat eye movement disorders, thus supplementing the treatment typically provided for concussed patients by the interdisciplinary team often including physical therapists (PTs), occupational therapists (OTs), and speech therapists. Learning how to collaborate with head-injury specialists can expand your practice’s offerings and, most important, provide a valuable service to patients.
KNOW YOUR NETWORK
If you are interested in growing this part of your practice, it is helpful to form relationships with referral sources, such as PTs and OTs at outpatient and inpatient rehabilitation facilities. Getting to know primary care physicians, providers at urgent care centers, and hospital emergency departments also helps to expand your network. Use meet-and-greet sessions as opportunities to educate these health care providers that eye movement disorders can be treated at your practice, and let them know that you are eager to collaborate.
Be sure to let these health care providers, particularly PTs and OTs, know that your aim is to complement, not to supplant, their care.
When speaking with health care practitioners, I remind them that neither physical therapy nor occupational therapy will help patients with eye movement disorders after brain trauma in totality. I educate them that sometimes the fix is very simple—say, adjusting the patient’s prescription or prescribing prism lenses—and I explain to PTs and OTs that a single visit to an optometrist may strengthen the care that they are providing or even help guide the course of care that they are providing.
INVESTMENTS
My office has offered vision therapy for post-concussion care for more than 5 years. In the past year, we have invested heavily in technology, staffing, and training in this area. One such investment was the RightEye tracking system (RightEye), which uses infrared eye tracking technology to provide objective measurement of eye movements. Before that investment, our office received approximately two brain injury–associated referrals each month; since that investment, we have received one or two such referrals a day. This investment has been our biggest source of new referrals in the past year, and has resulted in approximately $50,000 in increased revenue stream per year.
The RightEye tracking system quantifies eye movements that cannot be seen on routine examination and offers repeatable testing to evaluate a patient’s progress. By objectively assessing (and later reassessing) eye movements, pursuits, saccades, and fixation statuses, this platform can provide before and after readouts that may be used to help patients track their improvement (Figure). The patient’s neurologist, referring provider, PT, or OT may find the readouts helpful, too. Some readouts have even been helpful in accessing payment from insurers for vision rehabilitation and in litigation for auto insurance or workman’s compensation cases.
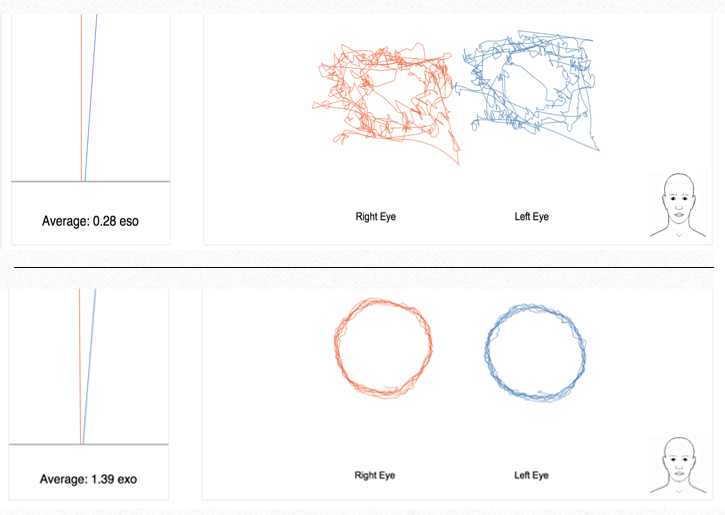
Figure. A readout from the RightEye tracking system shows the patient’s baseline fixation after brain injury (top) and after several weeks of therapy (bottom).
These patients are medically complex and highly motivated, and they often present with concurrent ocular pathology such as dry eye disease and glaucoma. Optometrists should be on the lookout for comorbidities when examining head trauma patients.
We optometrists got into this field to help patients in need, and patients with postconcussion syndrome are an important subset of patients that our field has largely ignored. Reinforcing our niche role in treating patients with postconcussion syndrome is an excellent practice-building strategy, and it can allow you to help numerous patients with recovery.

- Centers for Disease Control and Prevention. Traumatic Brain Injury in the United States. Published March 2010. www.cdc.gov/traumaticbraininjury/pdf/blue_book.pdf. Accessed November 28, 2018.
- Hagen S. The Mind’s Eye. The Rochester Review. 2012;72(4). http://www.rochester.edu/pr/Review/V74N4/0402_brainscience.html. Accessed November 28, 2018.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. Washington, DC: American Psychiatric Association; 1994.

