





Eye care professionals in the United States finally have a trifocal IOL to offer their patients undergoing cataract surgery. The AcrySof IQ PanOptix Trifocal IOL (Alcon), approved by the FDA last August, allows patients to see clearly at distance, intermediate, and near.
AT A GLANCE
- The AcrySof IQ PanOptix IOL can correct a patient’s distance, intermediate, and near vision, in addition to astigmatism with the toric version, at the time of cataract surgery.
- The availability of a trifocal IOL allows eye care professionals to simplify the education process with patients and streamline cataract evaluations.
- Although patients may still see halos at night, neural adaptation occurs over 3 to 6 months after surgery, resulting in high patient satisfaction.
Just 4 years ago we were unable to simultaneously correct astigmatism and presbyopia at the time of cataract surgery. Now the PanOptix IOL can correct a patient’s distance, intermediate, and near vision, in addition to astigmatism with the toric version (Figure). This technology has been available in markets outside the United States for more than 5 years, but we are going to take a look at how the PanOptix lens has performed inside the United States over the past year.
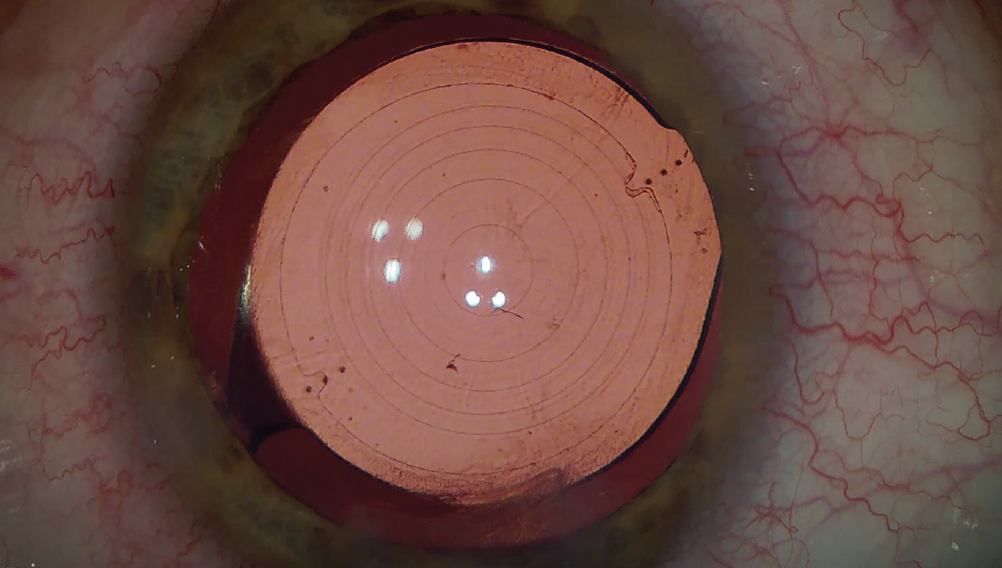
Figure. A toric PanOptix IOL immediately after refractive laser cataract surgery. As seen here, the IntelliAxis (LensAR) marks the anterior capsule to enable precise toric IOL alignment, allowing easy evaluation both intra- and postoperatively.
WHAT’S DIFFERENT?
At our practice, the PanOptix IOL has changed our approach to cataract surgery. Before the availability of a trifocal IOL, we used bifocal IOLs that were either high add (providing distance and near vision) or low add (providing distance and intermediate vision). Determining which of these best suited each patient’s daily activities could be both time-consuming and difficult.
Although many patients do well with a high add IOL in one eye and a low add in the fellow eye, convincing patients that they can do well with two different lenses in their eyes can add significant time to the education process. The trifocal IOL allows us to simplify our education process with patients and streamline our cataract evaluations.
HOW IS THE VISION?
The biggest benefit of the trifocal lens is the wide range of vision it provides. In our clinic, we routinely see patients with better than 20/25 vision at all ranges postoperatively. Multiple studies, including a recent one from Kohnen et al evaluating 1-year results, report great visual acuity results with the PanOptix IOL.1,2
Compared with bifocal IOLs, we spend less time postoperatively coaching patients where to hold reading material in order to see clearly with the trifocal. Instead, we can spend more time celebrating the fact that the patient can now see the TV, street signs, dashboard, computer, and phone without visual aids.
THE OPTICAL NITTY GRITTY
The PanOptix has a quadrifocal lens design but functions as a trifocal lens. This design provides focal points at 40 cm, 60 cm, 120 cm, and optical infinity. Using Alcon’s Enlighten technology, the extended intermediate focal point at 120 cm is redistributed to optical infinity in order to maximize patients’ distance vision. This technology allows the IOL to transmit 88% of light to the retina, a higher value than is achieved by other trifocal IOLs outside the US market.
WHAT ABOUT SIDE EFFECTS?
The PanOptix IOL is a diffractive trifocal, which means that patients will still see halos around point sources of light at night. The most obvious example would be seeing circles around headlights while driving at night. Patients should not expect to see those circles in environments with good lighting.
The good news is that the brain adapts to seeing these halos. Studies have found that during the first 3 to 6 months after surgery patients undergo neural adaptation so that they notice halos less and less. The aforementioned international multicenter study by Kohnen et al found that less than 5% of patients reported halos at the 1-year mark.1
PATIENT SELECTION
Who are the best candidates for a trifocal IOL? The easy answer is patients without ocular pathology looking for the return of good, binocular vision unencumbered by the need for reading glasses. Although this is true, it is not the full answer.
Patients must have good ocular health in order to be good candidates for a trifocal IOL. Retinal pathology that limits good central vision, such as macular degeneration or epiretinal membranes, is a common reason that a patient may not qualify for this lens. The ocular surface must also be in premium condition for premium visual results.
For patients with ocular surface conditions such as dry eye, epithelial basement membrane dystrophy, and Salzmann nodules, we recommend treating these conditions before determining if the patient is a good candidate for trifocal IOLs.
Presbyopic myopic patients can be challenging. Although the PanOptix IOL offers great near vision, for some patients it may not be equal to their most perfect near vision. Such patients must be aware that they might need to sacrifice a little of their near vision in order to obtain good distance and intermediate vision. The PanOptix IOL has been our best option in years for presbyopic myopic patients, but these patients require extra education to make sure they have appropriate expectations.
WHAT ABOUT refractive LENS EXCHANGE?
With the outstanding visual results reported with the PanOptix IOL, a number of our patients have elected to have refractive lens exchange (RLE). With trifocal IOLs in both eyes, these patients don’t have to wait for cataract surgery to enjoy good vision at all ranges.
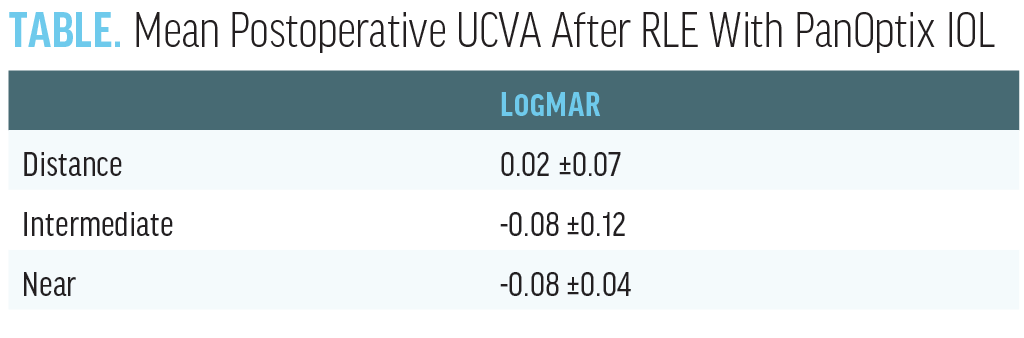
A retrospective review of our first 41 patients (82 eyes) who underwent RLE with the PanOptix IOL in both eyes found that 1 month postoperatively the mean uncorrected distance visual acuity (UDVA) was 0.02 ±0.07 LogMAR, mean uncorrected intermediate visual acuity (UIVA) was -0.08 ±0.12 LogMAR, and mean uncorrected near visual acuity (UNVA) was -0.08 ±0.04 LogMAR (Table). Of note, these patients were coming to us to improve their near vision, and all patients achieved UNVA of 20/20 or better postoperatively.
MORE TO COME?
Other IOLs that have some trifocality are on the way to market in the United States. The Tecnis Synergy IOL (Johnson & Johnson Vision), the Envista MX60EF IOL (Bausch + Lomb), the FineVision IOL (PhysIOL), and the AT LISA tri toric IOL (Carl Zeiss Meditec) could become available to our patients over the next 5 years. In fact, it is possible that we could have three trifocal options available in the United States by the end of 2021.
What About Extended Depth of Focus?
There is a role for extended depth of focus IOLs such as the Tecnis Symfony (Johnson & Johnson Vision) in some patients, but a trifocal lens gives patients a significantly increased amount of reading vision. For this reason, we don’t tend to use the Symfony in both eyes of our patients, just as we wouldn’t give a low-powered multifocal contact lens to a patient who wants great reading vision.
We have been keeping our eyes on trifocals over the past few years, looking at the European data, so the first day that the PanOptix IOL became available in the United States, Dr. Saenz had his mother get the lens in both eyes. We knew that this would be the best lens to give her the reading and intermediate vision she desired. Her VA is now better than 20/20 at all distances, and she loves her vision.
CASE REPORT
A nighttime truck driver with presbyopia walks into your clinic wanting spectacle independence. What solutions do you have?
A 59-year-old man presented to our clinic for a LASIK evaluation. His manifest refraction was +0.25 -3.75 x 087 OD and +1.25 -3.00 x 089 OS. He had a basal cell carcinoma on his nose, making the wearing of eyeglasses uncomfortable. We discussed refractive lens exchange to significantly reduce his dependence on glasses and educated him about halos at night, jokingly adding that it would only be an issue if he was a nighttime truck driver. His occupation? Nighttime truck driver!
We explained that, after surgery, he may not be able to drive at night. (We like to overdeliver on expectations.) We were hesitant to proceed with surgery due to his occupation, but after a lengthy discussion, the patient elected to have the PanOptix IOL implanted in both eyes.
His VA is better than 20/20 at distance, intermediate, and near 1 month after surgery, and he is still driving comfortably at night. He reports that he does see halos peripherally at night, but that they are not bothersome and that he loves his vision. In fact, this patient says more truck drivers should have this surgery!
TECHNOLOGY AT ITS BEST
There has never been a better time for patients to consider cataract surgery or RLE. In the PanOptix FDA clinical trial, 99% of patients said they would have the surgery again or recommend it to a family member. By providing the widest range of clear vision possible with minimal side effects, one can see why this lens creates so many happy patients. Optometrists should be aware of the capabilities of this new lens as changes in the health care environment place ever greater demands on optometrists for the pre- and postoperative care of cataract patients.
1. Kohnen T, Marchini G, Alfonso JF, et al. Innovative trifocal (quadrifocal) presbyopia-correcting IOLs: 1-year outcomes from an international multicenter study [published online ahead of print, April 30, 2020]. J Cataract Refract Surg.
2. Rementería-Capelo LA, Contreras I, García-Pérez JL, Blázquez V, Ruiz-Alcocer J. Visual quality and patient satisfaction with a trifocal intraocular lens and its new toric version. J Cataract Refract Surg. 2019;45(11):1584-1590.