


Management of glaucoma is centered on one modifiable risk factor: elevated IOP. Many methods have been used over the years to decrease aqueous production or increase aqueous outflow in order to lower IOP. These efforts have relied on the use of medications, laser application, or incisional surgery.
One versatile laser surgical procedure with a long history in glaucoma management is endoscopic cyclophotocoagulation (ECP). This procedure, combining endoscopic visualization with diode laser photocoagulation of the ciliary processes, was first described in 1992.1 ECP reduces aqueous production by means of direct ablation of the ciliary processes.2 Because the ciliary processes can be directly observed during the procedure, collateral tissue damage and postoperative pain are limited.3
Optometrists play a critical role in the education and referral process for ECP. They need to be well equipped to identify good candidates, properly educate the patient, provide contact with a qualified surgeon, and be able to manage the patient postoperatively.
INDICATIONS
ECP is a good option for treatment of patients with mild to moderate glaucoma, with IOPs of between 18 mm Hg and 30 mm Hg, who are already taking multiple glaucoma medications or who have not responded sufficiently to external filtration surgeries.4 It can be performed as a standalone procedure but is now more commonly combined with cataract surgery. This combination is a great option for those with visually significant cataracts who are interested in reducing their use of eye drops for the treatment of their glaucoma. When cataract surgery is performed before application of the laser, it not only eliminates the risk of the endoscope hitting the natural lens but also makes more room to access the ciliary sulcus.5
ECP has also been found to deepen the anterior chamber angle. Hollander et al investigated the effect of ECP on the anterior chamber angle in patients with plateau iris syndrome undergoing cataract extraction.6 The study authors found that areas treated with ECP showed open angles on gonioscopy and ultrasound biomicroscopy, whereas untreated areas in the same eye still showed iridociliary apposition.6
Pediatric glaucoma has also been successfully treated with ECP, although complications such as retinal detachment, hypotony, and progressive vision loss are more common in pediatric eyes.7
CONTRAINDICATIONS
In patients with pseudoexfoliative glaucoma, fibrillary buildup and stiffening of the ciliary processes result in less laser energy absorption by these tissues, adversely affecting ECP efficacy.4
In neovascular and uveitic glaucoma, ECP is more prone to cause severe postoperative inflammation.4 If however, treatment is necessary in these patients, less extensive application and more aggressive postoperative antiinflammatory treatment with intraocular or oral steroids can be implemented.
Another relative contraindication is IOP greater than 40 mm Hg.8 Patients with IOP this high may benefit more from a trabeculectomy or tube shunt glaucoma surgery than from ECP.
Note also that, if there is vitreous in the anterior chamber, it must be removed before laser application, as it will interfere with manipulation of the endoscope.9
PROCEDURE
The ciliary processes can be accessed either through the pars plana or via a limbal approach. The pars plana approach is performed less often because it requires an initial vitrectomy, but it can allow better visualization of the ciliary processes in aphakic or pseudophakic patients.8,10
Anesthesia can range from intracameral infusion to general anesthesia depending on the patient, the approach, and the surgeon’s requirements.4
The limbal approach typically requires a single corneal incision in a phakic, pseudophakic, or aphakic eye. Anterior chamber entry can be made either through a scleral tunnel or corneal incision; the latter preserves the conjunctiva for future filtering surgery if needed.3
An ophthalmic viscosurgical device (OVD) is used to expand the posterior chamber between the iris and the lens capsule. If ECP is combined with phacoemulsification, the cataract is removed before the laser application is performed.
The ECP procedure is performed using a handheld laser endoscope connected to a laser endoscopy unit (Endo Optiks Laser Endoscopy; BVI) (Figure 1). The handheld unit contains three optical fibers, incorporating an image guide, light guide, and laser guide.

Figure 1. Laser endoscope with curved probe.
The probe is inserted through the incision (Figure 2), and the surgeon views the procedure on a monitor and begins to apply laser to the ciliary processes. The energy is slowly increased until shrinkage and whitening of the ciliary processes can be seen (Figure 3).11
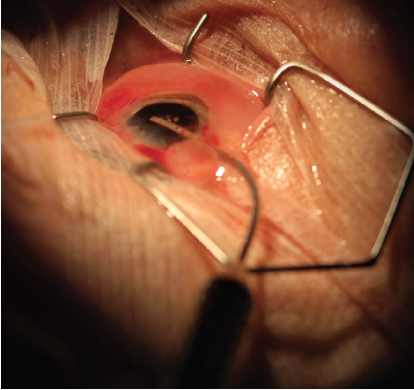
Figure 2. Laser endoscope probe inserted into the anterior chamber through a corneal incision.
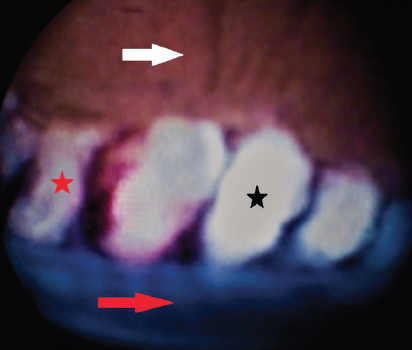
Figure 3. View of ciliary processes on the endoscopy unit monitor showing untreated ciliary process (red star), treated ciliary process with whitening (black star), posterior iris surface (white arrow), and anterior surface of lens capsule (red arrow).
One incision site can typically allow 270° of treatment. If more treatment is warranted, a second incision can be made 90° to 180° away. This allows access to the untreated ciliary processes and a complete 360° treatment.2 At the completion of the procedure, the surgeon removes the OVD to reduce postoperative IOP spikes.2
POSTOPERATIVE CARE
The most common complications after ECP include IOP spikes, fibrinous iritis, and hyphema.12 Less common complications can include retinal detachment, choroidal hemorrhage, vitritis, cystoid macular edema, hypotony, phthisis bulbi, and corneal decompensation.4,13
Postoperative care typically includes a topical antibiotic four times daily for 2 weeks, a topical nonsteroidal antiinflammatory agent four times daily for 1 to 2 weeks, and topical prednisolone acetate 1% every 2 hours while the patient is awake for 1 week with slow taper over 1 month. If further IOP and inflammation control is needed, oral acetazolamide and subconjunctival or sub-Tenon injections of a steroid may be used.14 The patient can use acetaminophen and short-term ice packs for comfort postoperatively.15
The patient should be seen for follow-up and IOP check at 1 day, 1 week, and 1 month after the procedure. Restrictions typically include avoiding eye rubbing and wearing a plastic or metal shield at bedtime for 1 week.
Patients should continue their preoperative regimen of IOP-lowering medications for 4 to 8 weeks after the ECP procedure.16 Once IOP has stabilized, one glaucoma drop may be discontinued at a time until an increase in IOP is observed.
EFFICACY
Since ECP was first introduced for the treatment of glaucoma, many authors have reported successful IOP reduction with the procedure. In a retrospective study, Chen et al reviewed the results of ECP in patients with a wide range of glaucoma etiologies, all of whom had not sufficiently responded to maximally tolerated medical therapy and many of whom had had one or more glaucoma surgeries. The study authors found that ECP reduced IOP by an average of 10.7 mm Hg (34%) and that in 90% of eyes postoperative IOP was less than 21 mm Hg.17
Phacoemulsification in combination with ECP has been shown to significantly increase the success rate of reducing IOP and reduce the need for glaucoma medications compared to phacoemulsification alone.18 Pérez Bartolomé et al compared a group that underwent phacoemulsification plus ECP with a group that underwent phacoemulsification alone; they found that 30% more patients in the combined group than in the phacoemulsification-only group achieved a 20% reduction in IOP.18
Another retrospective case review examined the differences in IOP reduction in patients undergoing ECP plus phacoemulsification who received one or two corneal incisions. In this report, Kahook et al found that the two-site procedures resulted in significantly larger reductions in IOP at 3- and 6-month follow-up visits compared to one-site procedures. They attributed the difference to having access to a larger treatment area with two incisions.12
A PLACE FOR ECP
ECP has been shown to be a viable option for patients with glaucoma on maximal therapy or for those who would like to reduce their dependence on topical medications. The precision this treatment allows, and the convenience it offers when performed in conjunction with phacoemulsification, make ECP an option that should be discussed with appropriate patients. When patients are properly educated about their choices, they can make the best decisions based on their lifestyles and needs.
1. Uram M. Ophthalmic laser microendoscope ciliary process ablation in the management of neovascular glaucoma. Ophthalmology. 1992;99(12):1823-1828.
2. Seibold LK, SooHoo JR, Kahook MY. Endoscopic cyclophotocoagulation. Middle East Afr J Ophthalmol. 2015;22(1):18-24.
3. Berke SJ. Endolaser cyclophotocoagulation in glaucoma management. Tech Ophthalmol. 2006;4(2):74-81.
4. Francis BA, Kwon J, Fellman R, et al. Endoscopic ophthalmic surgery of the anterior segment. Surv Ophthalmol. 2014;59(2):217-231.
5. Cohen A, Wong SH, Patel S, Tsai JC. Endoscopic cyclophotocoagulation for the treatment of glaucoma. Surv Ophthalmol. 2017;62(3):357-365.
6. Hollander DA, Pennesi ME, Alvarado JA. Management of plateau iris syndrome with cataract extraction and endoscopic cyclophotocoagulation. Exp Eye Res. 2017;158:190-194.
7. Neely DE, Plager DA. Endocyclophotocoagulation for management of difficult pediatric glaucomas. J AAPOS. 2001;5(4):221-229.
8. Kahook MY, Noecker RJ. Endoscopic cyclophotocoagulation. Glaucoma Today. 2006;4(6):24-29.
9. Uram M. Endoscopic Surgery in Ophthalmology. Lippincott Williams & Wilkins; 2003.
10. Huang JY, Lin S. Endoscopic cyclophotocoagulation. Glaucoma Today. 2009;7(2):38-41.
11. Dastiridou AI, Katsanos A, Denis P, et al. Cyclodestructive procedures in glaucoma: a review of current and emerging options. Adv Ther. 2018;35(12):2103-2127.
12. Kahook MY, Lathrop KL, Noecker RJ. One-site versus two-site endoscopic cyclophotocoagulation. J Glaucoma. 2007;16(6):527-530.
13. Beardsley R, Law SK, Caprioli J, et al. Comparison of outcomes between endoscopic and transcleral cyclophotocoagulation. Vision (Basel). 2017;1(4):24.
14. Rathi S, Radcliffe NM. Combined endocyclophotocoagulation and phacoemulsification in the management of moderate glaucoma. Surv Ophthalmol. 2017;62(5):712-715.
15. Gaasterland DE. Diode laser cyclophotocoagulation. Glaucoma Today. 2009;7(2):35-37, 41.
16. Fallano KA, Conner IP, Noecker RJ, Schuman JS. Cyclodestruction procedures in glaucoma. In: Yanoff M, ed. Ophthalmology, 5th ed. Elsevier; 2019:1131-1134.
17. Chen J, Cohn RA, Lin SC, Cortes AE, Alvarado JA. Endoscopic photocoagulation of the ciliary body for treatment of refractory glaucomas. Am J Ophthalmol. 1997;124(6):787-796.
18. Pérez Bartolomé F, Rodrigues IA, Goyal S, et al. Phacoemulsification plus endoscopic cyclophotocoagulation versus phacoemulsification alone in primary open-angle glaucoma. Eur J Ophthalmol. 2018;28(2):168-174.

