

Meibomian gland dysfunction (MGD), one of the leading causes of dry eye disease, is characterized by decreased and thickened secretion from the oil-producing glands of the tear film.1 MGD decreases not only the quality of the oil secretions, but also the quantity of working glands. These oil glands help to produce the lipid layer of the tear film, and compromise to this layer can cause severe discomfort for a patient. The best approach to relieve meibomian gland obstruction includes applying heat to the eyelids. While warm compresses and physical massage to the external eyelids has been the traditional approach to improving oil flow, it is not the most effective and requires reheating for optimal results.2 Warm compresses and physical eyelid massage have been shown to change the shape of the cornea, which could cause secondary keratoconus and other corneal irregularities that may decrease a patient’s overall visual acuity.3 »LipiFlow Thermal Pulsation System (Johnson & Johnson Vision) both heats and pulsates the meibomian glands from the internal eyelid surface without compromising the cornea. Patients’ symptoms and oil gland function have been shown to improve for up to 9 months after treatment.4
CASE HISTORY
A 42-year-old woman presented for an annual eye examination with a chief complaint of fluctuating vision at both distant and near. She has a history over the last several years of dryness in both eyes, but all other ocular and medical history is negative. Omega-3 supplementation and »Restasis (cyclosporine; Allergan) had been previously recommended, but the patient had poor compliance. A SPEED/OSDI questionnaire revealed scores of 19 and 18, respectively (a normal SPEED score is <10; a normal OSDI score is <20).
EXAMINATION
Examination revealed BCVA of 20/30- OD, 20/25- OS. Slit-lamp examination revealed thickened, inspissated oil expression in both eyes with reduced tear film break-up time with sodium fluorescein (NaFl) staining. Posterior segment findings were unremarkable. It was recommended the patient return at her earliest convenience for a dry eye evaluation and restart 1000 mg of EPA/DHA omega-3 fatty acid supplementation per day.
Further testing of dry eye revealed meibomian gland atrophy as graded by the Meibo scale using the Oculus »Keratograph 5M. The lower and upper eyelids were 3.5 in both eyes (Figure 1), indicating greater than 75% of meibomian gland atrophy. Further testing revealed a decreased noninvasive tear film break-up time of 6.78 seconds (Figure 2). Lissamine green stain revealed a moderate Line of Marx in both eyes, superiorly and inferiorly. Lid Wiper Epitheliopathy was 3×2 in each eye. The number of meibomian glands yielding liquid secretion (MGYLS) was also evaluated, performed on the lower eyelids with a meibomian gland expressor (constant pressure of 1.25 mm/g2). The total MGYLS score was 5 OD and 5 OS.
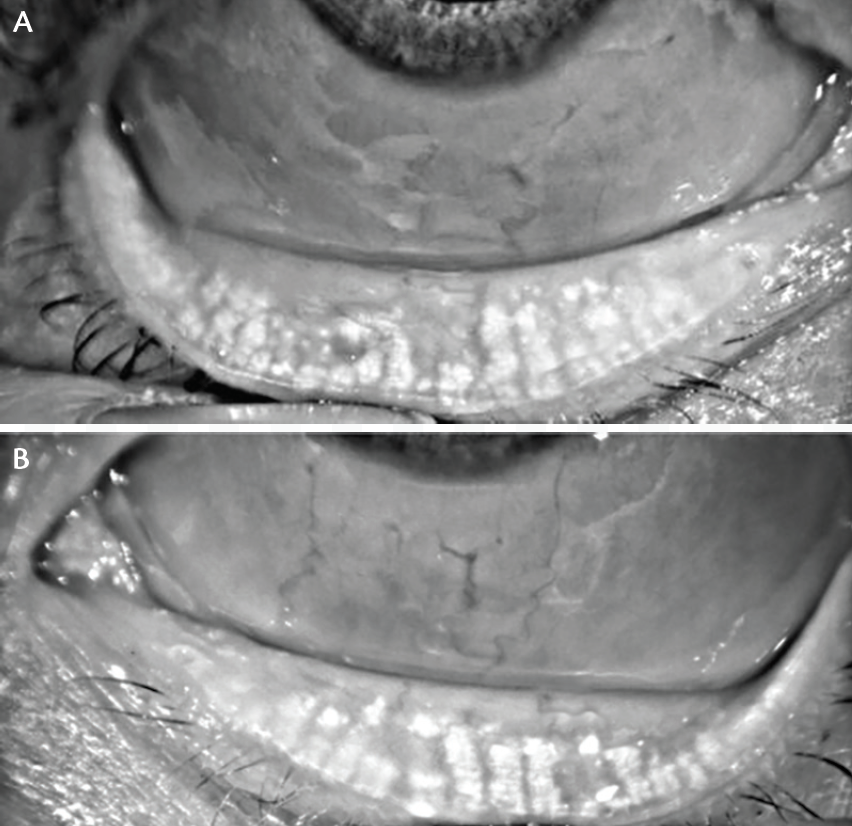
Figure 1. Meibography of left lower lid (A) and right lower lid (B) was tested with the Oculus Keratograph 5M, revealing a grade of 3.5, representing greater than 75% meibomian gland atrophy.
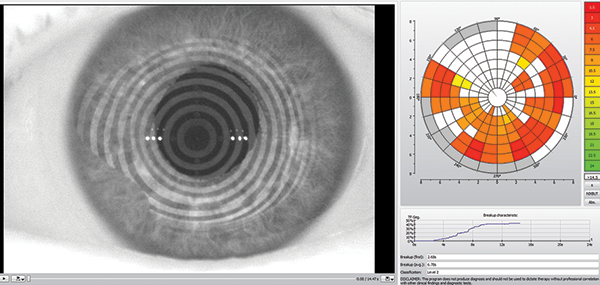
Figure 2. Testing with the Oculus Keratograph 5M revealed a noninvasive tear film break-up time of 6.78 seconds.
DIAGNOSIS
MGD
TREATMENT AND OUTCOME
Based on severity of dry eye signs and symptoms, LipiFlow was performed in office. The patient was instructed to restart Restasis twice daily OU, 1000 mg EPA/DHA omega-3 fish oils, and perform nightly warm compresses. At follow-up appointment 4 weeks after LipiFlow, the patient reported very little relief of her dry eye symptoms. However, her SPEED/OSDI scores were 14/10, indicating improvement from previous scores. Total MGYLS scores were 18 OD and 14 OS. Although MGYLS improved drastically since the initial evaluation, the patient was concerned that LipiFlow did not completely cure her dry eye symptoms. It was recommended the patient continue blinking exercises, warm compresses, and artificial tears as needed.
At the next follow-up appointment at 6 weeks after LipiFlow treatment, the patient’s symptoms had improved dramatically since her previous visit with a SPEED/OSDI of 8/7. BCVA was 20/20 OD and OS. Her noninvasive tear film break-up time drastically improved to 24.0 seconds (Figure 3). Furthermore, her MGYLS score was 20 OD and 22 OS. It was recommended the patient continue Restasis twice daily OU, the omega-3 fatty acid supplement, and warm compresses for 10 minutes a day.
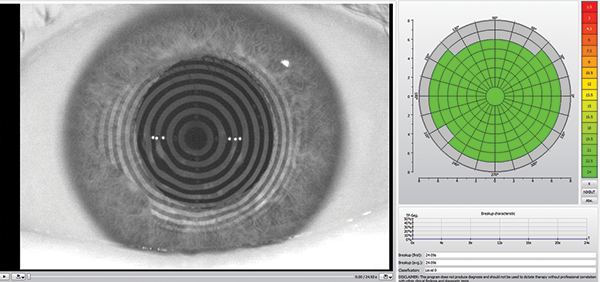
Figure 3. After treatment, the patient’s noninvasive tear film break-up time drastically improved to 24.0 seconds, as shown here on the Oculus Keratograph 5M.
CONCLUSION
The Oculus Keratograph 5M provides many features that are useful for obtaining dry eye data for patients, including meibography, noninvasive tear film break-up time, bulbar and limbal redness evaluation, and tear meniscus height. The accuracy and consistency provided by this instrument is highly valuable in providing the best care for my dry eye patients.
- Blackie CA, Carlson AN, Korb DR. Treatment for meibomian gland dysfunction and dry eye symptoms with a single-dose vectored thermal pulsation. Curr Opin Ophthalmol. 2015;26(4):306-313.
- Blackie CA, Solomon JD, Greiner JV, et al. Inner Eyelid Surface Temperature as a Function of Warm Compress Methodology. Optom Vis Sci. 2008;85(8): 675-683.
- Mcmonnies CW, Korb DR, Blackie CA. The role of heat in rubbing and massage-related corneal deformation. Cont Lens Anterior Eye. 2012;35(4):148-154.
- Greiner JV. A single LipiFlow Thermal Pulsation System treatment improves meibomian gland function and reduces dry eye symptoms for 9 months. Curr Eye Res. 2012;37(4):272-278.

