Refractive surgery has advanced greatly since the early days of the field’s founders, José Ignacio Barraquer, MD, and Svyatoslov Fyodorov, MD. Keratomileusis, radial keratotomy, conductive keratoplasty, epikeratophakia, and automated lamellar keratoplasty are among the refractive procedures that were used previously but cannot meet the stringent standards of today.
Commonly performed types of refractive surgical procedures now include LASIK, PRK, phakic IOLs, corneal inlays, corneal strengthening procedures (corneal collagen crosslinking and intrastromal corneal ring segments), refractive lens exchange/cataract surgery, and, most recently, small-incision lenticule extraction (SMILE).
SMILE ENTERS THE ARENA
SMILE is the newest form of laser vision correction (LVC). It has many similarities to LASIK, but also important differences. The concept of lenticule removal was first reported in 2008, but it wasn’t until more recently that femtosecond laser technology improved to the point that the procedure could produce the excellent results we see today.1 The first US clinical trials for SMILE began in June 2012.2 Since then, more than 1 million procedures have been performed worldwide, and the number of patients undergoing SMILE is rising rapidly.3
WHAT TO KNOW: LASIK VS. SMILE
Because optometrists are often the first eye care professionals to encounter patients who are interested in LVC, it is important for them to know the differences between SMILE and LASIK (Table). Here are three major differences between the two procedures.
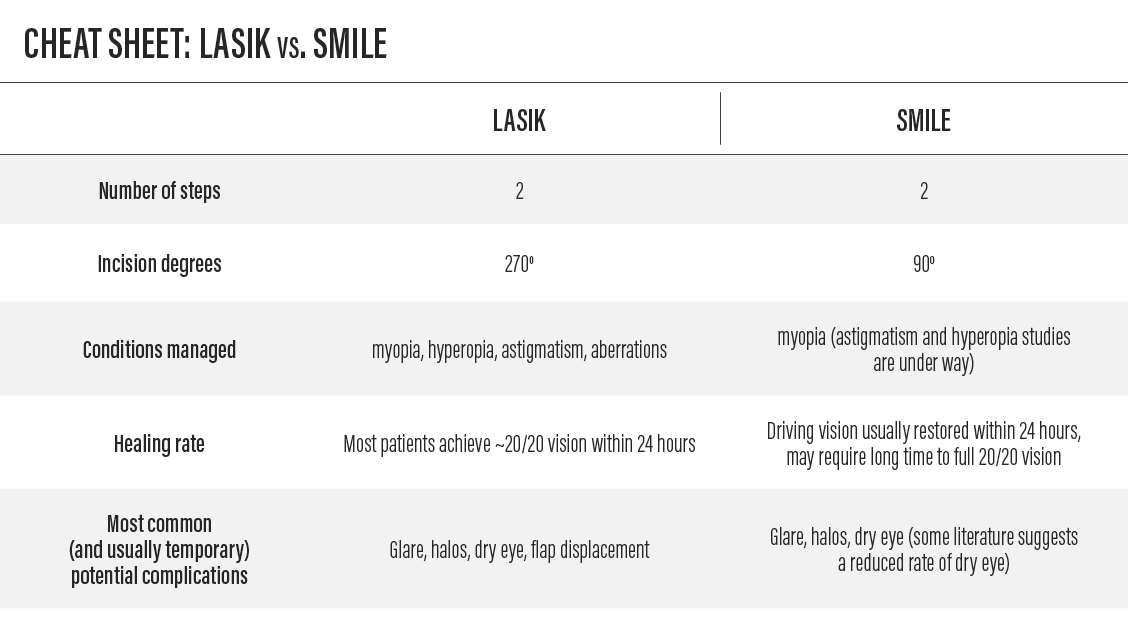
Table. There are a few important differences between LASIK and SMILE. Patients are most likely to be concerned with healing rate and potential complications.
Difference No. 1: Procedure
LASIK is a two-step procedure. The first step involves creation of a thin corneal flap with either a femtosecond laser or a mechanical microkeratome. In the second step, the flap is lifted and excimer laser ablation reshapes the underlying corneal stroma to treat the patient’s particular ametropia. The flap is then repositioned and acts as a natural bandage, allowing rapid visual recovery. Of note, three significant ablation patterns advancements (wavefront-optimized, wavefront-guided, and topography-guided) have been developed in recent years to improve visual outcomes to the level we achieve today. All have their benefits and weaknesses, but they all have improve the level of vision beyond those of more traditional treatments.
SMILE is also a two-step procedure. First, a femtosecond laser creates two intrastromal cuts, rather than the single cut required in LASIK. There is first a posterior refractive cut, followed by an anterior cap cut that creates an intrastromal lenticule. A small opening is then made to allow access to the newly created lenticule. In the second step, the lenticule is manually dissected and removed, resulting in a reshaped cornea to treat the patient’s ametropia. This lenticule shape is created in a wavefront-optimized fashion, allowing excellent quality of vision similar to wavefront-optimized LASIK.
Difference No. 2: Refractive Conditions Treated
Both LASIK and SMILE have been heavily studied and shown to be safe and effective with high levels of patient satisfaction.
LASIK can treat a wide range of refractive errors, including myopia, hyperopia, astigmatism, and, in some cases, higher-order aberrations.
In the United States, SMILE is approved to treat myopia from -1.00 D to -8.00 D with up to -0.50 D of myopic astigmatism. Use of SMILE to address astigmatism and hyperopia is being studied in international trials, and it is expected that SMILE will be used to manage these conditions in the United States in the future.
Difference No. 3: Postoperative Period
LASIK and SMILE have similar postoperative courses. A good rule of thumb for most refractive procedures is that full visual recovery can be achieved within 3 to 6 months. Functional visual recovery is rapid for patients who undergo either procedure, and most patients obtain legal driving vision within 24 hours of either procedure. It should be noted that LASIK patients typically obtain 20/20 vision on the day after the procedure, but SMILE patients may have to wait slightly longer to achieve a full 20/20 result.
Complications of LASIK and SMILE are rare and often resolve themselves; they can include glare, halos, and eye dryness. The most significant difference in the postoperative period concerns dry eye: because SMILE affects the subbasal corneal nerve plexus less than LASIK, less dry eye occurs during the first 3 to 6 months of the postoperative period.4 In addition, because no flap is present with SMILE, the risk of dislocation is lower than with LASIK.
ODs ON THE FRONT LINE
As a surgeon, I can tell you that a patient who is educated on the differences among LVC options makes my job easier: I can spend more time in the OR and less time imparting information to that patient. Arming yourself with these few facts benefits patients and helps to bolster the collaborative foundations of eye care.

- Sekundo W, Kunert K, RussmannD, et al. First efficacy and safety study of femtosecond lenticule extraction for the correction of myopia: six-month results. J Cataract Refract Surg. 2008;34(9):1513-1520.
- Randomized, non-inferiority trial comparing SMILE and LASIK. ClinicalTrials.gov. https://clinicaltrials.gov/ct2/show/NCT01216475. Accessed January 22, 2018.
- Zeiss celebrates 1 million SMILE laser vision correction procedures [press release]. Jena, Germany: Zeiss; September 28, 2017.
- Reinstein DZ, Archer TJ, Gobbe M. Small incision lenticule extraction (SMILE) history, fundamentals of a few refractive surgery technique and clinical outcomes. Eye and Vis. 2014;1(3).