Scleral lenses have become an increasingly popular and successful option for patients with irregular corneas due to ectasia, surgery, ocular surface disease, or scarring after trauma or infection. With advances in materials and lathe technology, the reproducibility and customization of scleral lenses has improved dramatically since early versions, resulting in healthier lens wear.1 Although it seems these innovations have yielded lenses that can be modified to work well for even the most challenging eyes, there are situations in which scleral lens specialists should exercise extra caution. The following are case examples to help illustrate this.
CASE No. 1: CORNEAL GRAFT AND APHAKIA
With the availability of scleral lenses in oblate designs, we are now able to better match the shape of the cornea after penetrating keratoplasty. However, patients with grafts may have low endothelial cell counts, which can make them more susceptible to adverse hypoxic sequelae.2 The minimum recommended endothelial cell count for considering scleral lens fitting is 800 cells/mm2.3 Clinicians may minimize risk by selecting a hyper-Dk material and requesting a center thickness as thin as possible, but options may be limited depending on the required power and design of the lens. Caution is advised for patients with corneal edema after penetrating keratoplasty. A different contact lens modality—such as a corneal gas permeable lens—may be indicated for some patients.
Patient Profile
A 64-year-old Indian woman presented with a history of fungal infection after cataract extraction and aphakia with a decentered graft OS (Figure 1). She was managed by a cornea specialist and was referred for scleral lens fitting. The thickness of her scleral lens was greater than desired—0.74 mm—due to the high hyperopic lens power of +18.50 D. Despite a hyper-Dk material and minimized clearance, persistent mild graft edema was seen after 3 to 6 hours of wear. The patient appreciated the comfort and vision with the lens, and she may be better suited for an impression-mold design, such as the EyePrintPRO (EyePrint Prosthetics), a lens that precisely matches the anterior ocular surface and can achieve a thinner overall thickness.4
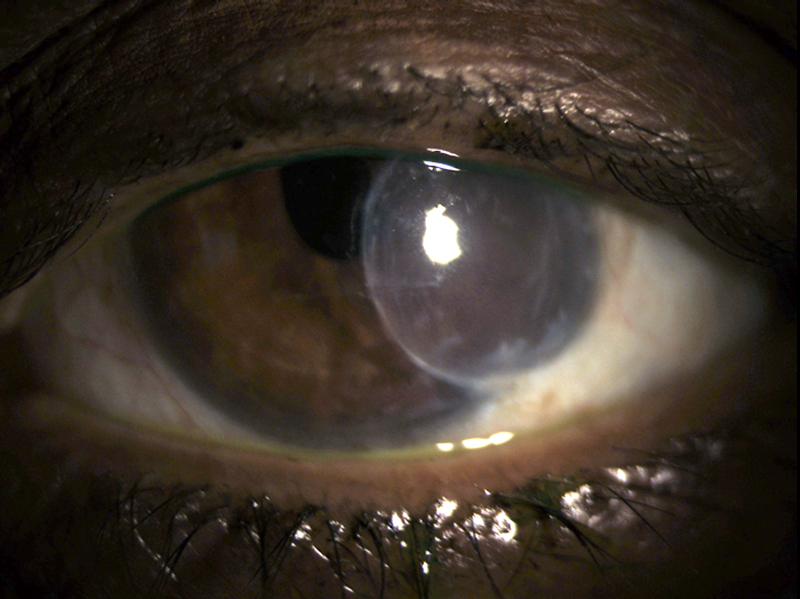
Figure 1. An aphakic patient with a decentered corneal graft.
CASE No. 2: GLAUCOMA WITH FILTERING BLEB
Increasing options for modifying the haptic portion of a scleral lens—including the addition of toric peripheral curves, notching, and vaulting—have allowed successful scleral lens fitting in patients with challenging conjunctival conditions. Although it may be acceptable for the haptic to lightly rest upon relatively benign lesions such as pingueculae, pressure on a bleb may result in reducing the bleb’s ability to lower IOP.5,6
Patient Profile
A 64-year-old white man with low vision presented with a history of microcornea, nystagmus, and congenital glaucoma with a large, elevated filtering bleb OD (Figure 2). His best corrected vision with spectacles was 20/150 OD and light perception OS. There was marked improvement in quality of vision (although there was no acuity improvement) when a corneal gas permeable lens was applied to the right eye, but the lens was unstable and uncomfortable due to his nystagmus.
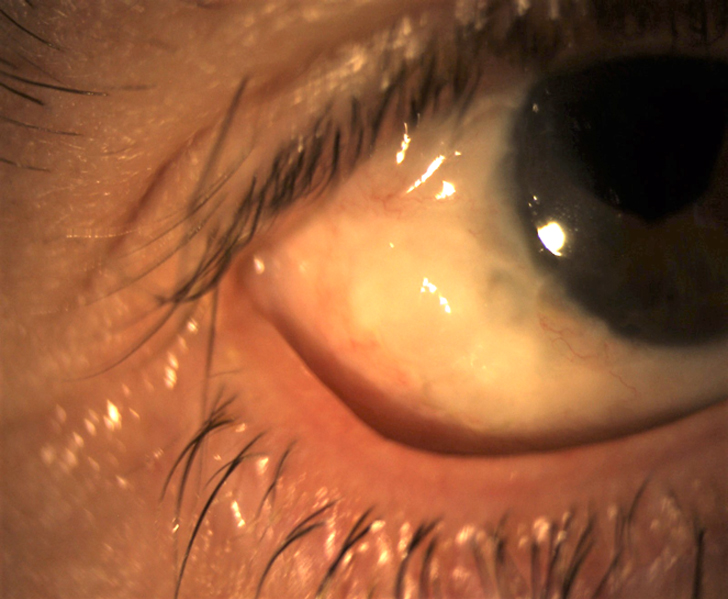
Figure 2. This patient’s microcornea, nystagmus, and bleb presented a challenge to scleral lens fitting.
The patient was refit into a small-diameter corneoscleral lens. The patient was comfortable, but the lens continued to land on the bleb despite several haptic modifications. After consulting with the patient’s glaucoma specialist, it was mutually decided that the best option would be to avoid the bleb completely. The area of the lens over the bleb was measured, and a notch was carved out. In a de facto monocular patient, it is critical to communicate with the comanaging ophthalmologist to ensure good health of the remaining eye.
CASE No. 3: EXTENDED WEAR
Some of the most challenging patients scleral lens fitters face are those who are noncompliant, whether through negligence, lack of education, or some combination. Patient education is crucial in achieving long-lasting and healthy scleral lens wear. Even a well-fit lens can result in damaging sequelae if it is not worn and cared for appropriately. Indeed, poor scleral lens handling is one of the most common reasons for complications of scleral lens wear.7
Patient Profile
A 21-year-old Pacific Islander woman with a history of advanced keratoconus was successfully fit with scleral lenses. At her initial scleral lens dispensing appointment, she was trained on application, removal, care, and handling of her scleral lenses. She was given written instructions for proper protocol, which included not sleeping in the lenses, and was told to return for routine follow-up. Despite multiple attempts to contact the patient, she did not return for nearly a year. It was discovered the patient had been wearing her lenses on an extended-wear basis, which resulted in severe corneal neovascularization extending into the visual axis OU (Figure 3). The patient was instructed to see a corneal specialist.
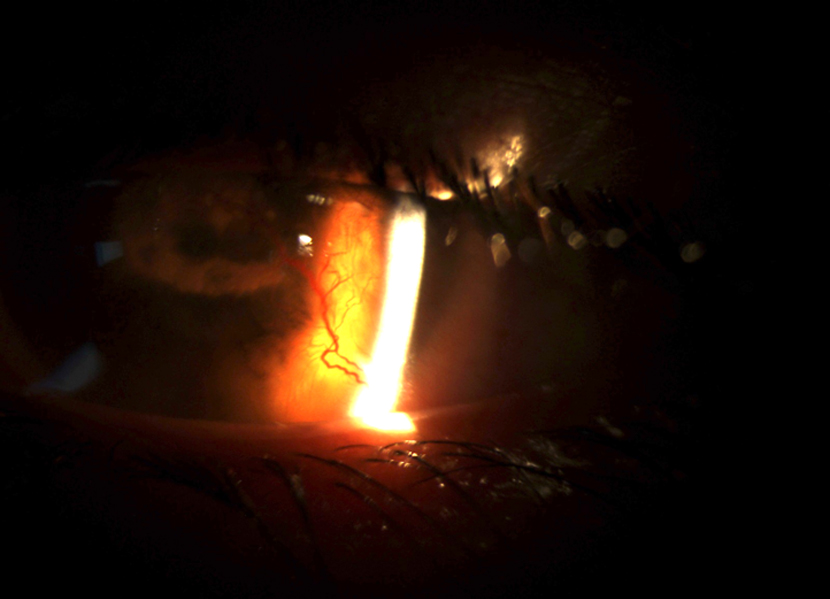
Figure 3. Extensive corneal neovascularization after extended wear of scleral lenses.
UNCOMMON, BUT NOT UNHEARD OF
These examples represent uncommon situations that require special care when initiating a scleral lens fitting, and it is prudent to be aware of such cases. As optometrists fit an increasing number of scleral lenses, we must be cautious when using them in populations that present increased risk for complications, such as pediatric and monocular patients. Caution is also needed when scleral lenses are to be used on a temporary extended-wear basis to address severe ocular surface disease.8-11
In normal eyes, the scleral lens fitter must weigh risks against benefits. A good deal of research on scleral lenses is under way, and more is needed to truly understand if there are long-term effects on the physiology of the eye so that we can confidently and responsibly continue to use this revolutionary technology.

- Rathi V, Mandathara P, Taneja M, et al. Scleral lens for keratoconus: technology update. Clin Ophthalmol. 2015;9:2013-2018.
- Jonuscheit S, Doughty MJ, Ramaesh K. The corneal endothelium after keratoplasty for keratoconus. Clin Exp Optom. 2013;96(2):201-207.
- Worp EV. A Guide to Scleral Lens Fitting. 2nd ed. Forest Grove, OR: Pacific University; 2015.
- Nguyen MTB, Thakrar V, Chan CC. EyePrintPRO therapeutic scleral contact lens: indications and outcomes. Can J Ophthalmol. 2018;53(1):66-70.
- Tanhehco T, Jacobs DS. Technological advances shaping scleral lenses: the Boston ocular surface prosthesis in patients with glaucoma tubes and trabeculectomies. Semin Ophthalmol. 2010;25(5-6):233-238.
- Nguyen AH, Dastiridou AI, Chiu GB, et al. Glaucoma surgical considerations for PROSE lens use in patients with ocular surface disease. Cont Lens Anterior Eye. 2016;39(4):257-261.
- Barnett M, Toabe M. Chapter 13: Scleral Lens Handling. In: Barnett M, Johns LK, eds. Contemporary Scleral Lenses: Theory and Application. Vol. 4. Sharjah, UAE: Bentham Science Publishers; 2017.
- Rathi VM, Mandathara PS, Vaddavalli PK. Fluid filled scleral contact lens in pediatric patients: challenges and outcome. Cont Lens Anterior Eye. 2012;35(4):189-192.
- Rosenthal P, Cotter JM, Baum J. Treatment of persistent corneal epithelial defect with extended wear of a fluid-ventilated gas-permeable scleral contact lens. Am J Ophthalmol. 2000;130(1):33-41.
- Smith GT, Mireskandari K, Pullum KW. Corneal swelling with overnight wear of scleral contact lenses. Cornea. 2004;23(1)29-34.
- Ciralsky JB, Chapman KO, Rosenblatt MI. Treatment of refractory persistent corneal epithelial defects: a standardized approach using continuous wear PROSE therapy. Ocul Immunol Inflamm. 2015;23(3):219-224.