



Small incision lenticule extraction (SMILE) has recently become the latest surgical option for nearsighted patients in the United States, expanding the menu of refractive surgery procedures that has included LASIK, PRK, and phakic IOL implantation.
New refractive surgery treatments broaden the patient eligibility pool, and refractive surgery comanagement has become fundamental to the core curriculum at contemporary optometry schools. Full-scope optometrists will play an increasingly large role in managing refractive surgery patients as the popularity of this vision-correction option continues to grow. Optometrists who feel confident discussing SMILE when patients ask about refractive surgery options put themselves and their patients at an advantage over others.
WHAT IS SMILE?
In SMILE, myopia is corrected with a femtosecond laser (»VisuMax, Carl Zeiss Meditec). The laser creates a refractive lenticule, which is then extracted through a small opening in the anterior stroma. The removal of this small sliver of tissue effectively flattens the too-steep central cornea, similar to an excimer laser ablation in PRK or LASIK.1
SMILE is considered a microinvasive procedure; it could be fairly compared with laparoscopic joint surgery. No flap is created during SMILE, and it requires only a femtosecond laser system, no excimer laser as in femtosecond-assisted LASIK. The structural integrity of Bowman layer and most of the anterior stroma is preserved.
One benefit of SMILE is that the cornea is biomechanically stronger.2-5 Also, because fewer corneal nerves are interrupted, SMILE may result in less short-term dry eye disease than is seen after PRK and LASIK,6-8 although recent research has shown that patients have fewer dry eye symptoms after modern LASIK compared with staying in their contact lenses.9
Watch a SMILE Procedure in Less Than 30 Seconds
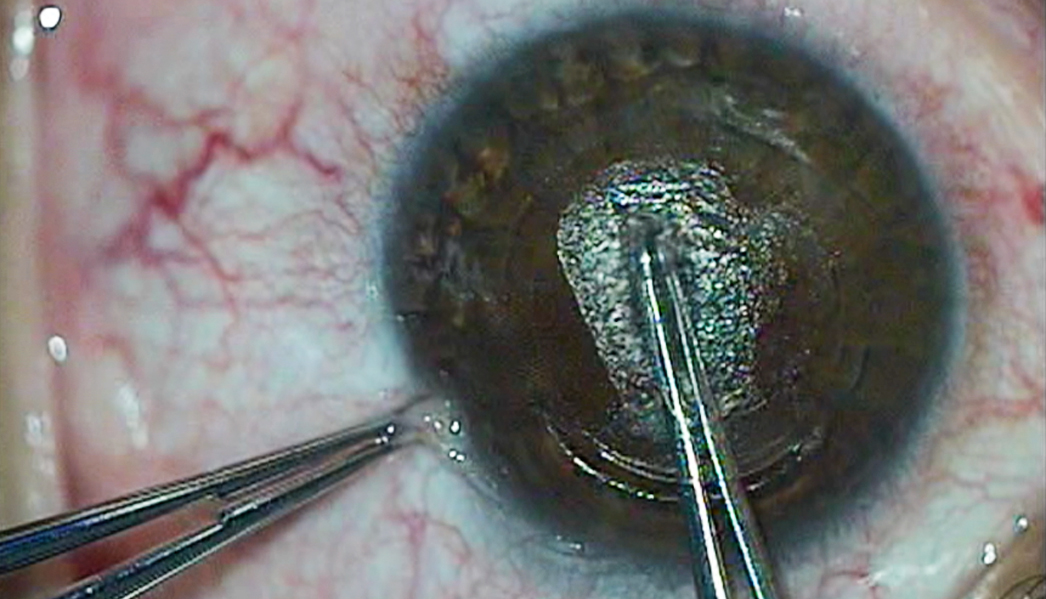
Figure 1. A lenticule is removed during SMILE.
Bobby Saenz, OD, MS, FAAO, offers a crash course in small incision lenticule extraction (SMILE), guiding viewers through a surgery performed by Gregory D. Parkhurst, MD, FACS. Dr. Saenz shows how Dr. Parkhurst relies on a VisuMax laser (Carl Zeiss Meditec) to define the lenticule, and explains the postoperative regimen and outlines candidates for SMILE. The juiciest part? Dr. Parkhust demonstrates how a lenticule is removed via a small incision (Figure 1).
Drs. Saenz and Parkhurst uploaded this video to the optometry channel on Eyetube, an online video resource for eye care providers. Watch their video here.
CANDIDATES
The FDA approved the VisuMax laser to perform the SMILE procedure for treatment of myopia of -1.00 D to -10.00 D with up to 0.50 D of cylinder. Outside the United States, SMILE has been used to treat hyperopia and up to 5.00 D of cylinder.
We find that many primary care optometrists want to know the minimum corneal thickness needed in order to recommend SMILE. The answer is easy: The same principles that apply to LASIK also apply to SMILE. If the patient’s corneal thickness is greater than 490 µm and there will be sufficient residual bed thickness based on the patient’s preexisting refractive error, the optometrist may discuss SMILE as a refractive option with this patient.
Patients most likely to choose SMILE are generally those who are early technology adopters. Patients who fear refractive surgery due to concerns about possible flap complications (even when they have been told that such complications are exceedingly rare with modern LASIK) may also be good candidates for SMILE.
IS SMILE SAFE?
SMILE and LASIK has been shown to be comparable in safety and efficacy.6 Blum et al showed that, over 5 years, SMILE was an effective, stable, and safe procedure for treating myopia and myopic astigmatism.10
Patients often feel reassured when they hear that more than 1 million SMILE cases have been performed. Even though the first case was performed in 2006, SMILE was approved in the United States in September 2016.
POSTOPERATIVE CARE
Postoperative comanagement of SMILE patients and LASIK patients is similar. Patients are instructed to use postoperative steroid and broad-spectrum antibiotic drops four times a day for 1 week; some clinicians advise that they use the drops for 2 weeks. Postoperative visits occur at 1 day, 1 week, and 1 month.
SMILE patients experience rapid visual recovery. Recovery time after SMILE is shorter than after PRK but slightly longer than after LASIK. Patients who know that their vision will continue to improve during the first few postoperative weeks, and therefore are prepared for this postoperative waiting period, are less likely to be disappointed with their immediate visual outcomes in the postoperative period.
WHAT’S COMING DOWN THE PIPELINE?
The optometrist is usually the first clinician to learn that a patient wants to reduce his or her dependence on glasses. It is imperative that ODs continue to educate themselves on the important facts of SMILE so that they can communicate to patients the options that are available.
If and when SMILE is approved by US regulators to treat astigmatism up to 5.00 D, we believe that more patients will choose SMILE. This means that optometrists must be ready to educate patients before the procedure and care for them afterwards.


- Sekundo W, Kunert KS, Blum M. Small incision corneal refractive surgery using the small incision lenticule extraction (SMILE) procedure for the correction of myopia and myopic astigmatism: results of a 6 month prospective study. Br J Ophthalmol. 2011;95:335-339.
- Wang D, Liu M, Chen Y, et al. Differences in the corneal biomechanical changes after SMILE and LASIK. J Refract Surg. 2014;30:702-707.
- Wu D, Wang Y, Zhang L, Wei S, Tang X. Corneal biomechanical effects: small-incision lenticule extraction versus femtosecond laser-assisted laser in situ keratomileusis. J Cataract Refract Surg. 2014;40:954-962.
- Osman IM, Helaly HA, Abdalla M, Shousha MA. Corneal biomechanical changes in eyes with small incision lenticule extraction and laser assisted in situ keratomileusis. BMC Ophthalmol. 2016;16:123.
- Shetty R, Francis M, Shroff R, et al. Corneal Biomechanical changes and tissue remodeling after SMILE and LASIK. Invest Ophthalmol Vis Sci. 2017;58(13):5703-5712.
- Zhang Y, Shen Q, Jia Y, et al. Clinical outcomes of SMILE and FS-LASIK used to treat myopia: a meta-analysis. J Refract Surg. 2016;32(4):256-265.
- Shen Z, Shi K, Yu Y, et al. Small incision lenticule extraction (SMILE) versus femtosecond laser-assisted in situ keratomileusis (FS-LASIK) for myopia: a systematic review and meta-analysis. PLoS One. 2016;11(7):e0158176.
- Cai WT, Liu QY, Ren CD, et al. Dry eye and corneal sensitivity after small incision lenticule extraction and femtosecond laser-assisted in situ keratomileusis: a meta-analysis. Int J Ophthalmol. 2017;10(4):632-638.
- Price MO, Price DA, Bucci FA Jr, et al. Three-year longitudinal survey comparing visual satisfaction with LASIK and contact lenses. Ophthalmology. 2016;123(8):1659–1666.
- Blum M, Täubig K, Gruhn C, et al. Five-year results of small incision lenticule extraction (ReLEx SMILE). Br J Ophthalmol. 2016;100(9):1192-1195.

