Oral omega-3 supplements were no better than placebo in relieving the signs and symptoms of dry eye disease (DED) in a clinical trial funded by the National Eye Institute.1 The Dry Eye Assessment and Management (DREAM) study was the first large-scale, real-world randomized clinical trial to study the long-term efficacy and safety of omega-3 supplements for patients with symptomatic DED.
These findings clash with the practices of many eye care clinicians who recommend omega-3 supplements to their patients for the relief of DED symptoms, but the findings are in line with the AAO’s Preferred Practice Pattern for DED, which states that “evidence is insufficient to establish the effectiveness of any particular formulation” of omega-3 fatty acid supplement to combat the disorder.2
The 3-year, 27-center DREAM study was led by researchers at the Perelman School of Medicine at the University of Pennsylvania and the Icahn School of Medicine at Mount Sinai in New York. The researchers enrolled 535 people with at least a 6-month history of moderate to severe DED, and all were randomly assigned to receive either a daily omega-3 supplement or an olive oil placebo. Each omega-3 dose contained 2,000 mg of eicosapentaenoic acid (EPA) and 1,000 mg of docosahexaenoic acid (DHA). Each placebo dose contained 5 g of olive oil, equal to approximately 1 tsp. A total of 186 participants received the daily doses of olive oil. The supplements and placebos were delivered in identical capsules, and neither patients nor providers knew which they were receiving. After 12 months, the researchers found that participants’ symptoms had improved substantially in both groups, but there was no significant difference in the degree of symptom improvement between the groups.
The primary outcome was the mean change from baseline in Ocular Surface Disease Index (OSDI) score. Secondary outcomes included the following: the proportion of patients with a decrease from baseline in OSDI score of 10 points or more, changes in the percentage of EPA and DHA in total fatty acids in red blood cells, changes in signs of DED based on conjunctival staining score, tear breakup time (TBUT), and Schirmer test results.
The researchers reported that 61% of people in the omega-3 group and 54% in the control group achieved at least a 10-point improvement in OSDI symptom score, but the difference between the groups was not statistically significant.1
REAL-WORLD TRIAL
Penny A. Asbell, MD, FACS, MBA, FARVO, a professor of ophthalmology at the Icahn School of Medicine at Mount Sinai, was the chair of the DREAM study. “The study was designed to be a real-world trial,” she said in an interview with Bryn Mawr Communications, the publisher of CollaborativeEYE. “The way we use omega-3 in practice, typically, is as an add-on. Most practitioners do not use omega-3 as a first-line treatment. They tell patients, ‘Try an artificial tear, or maybe a prescription immunomodulator. If those don’t work, maybe we will add on omega-3.’ Based on that real-world model, we included people who would typically present at an eye care provider with complaints of dry eye symptoms despite being on other treatments for DED. These are the kinds of people who most of us see every day in clinical practice.”
Dr. Asbell said patients in the study were randomly assigned to treatment or placebo, “while they continued doing whatever else they were doing for their dry eyes. We added on, and in that sense it reflects real-world behaviors.”
Dr. Asbell continued, “This is quite different from an industry-sponsored trial for new drug approval by the FDA, where restrictive inclusion and exclusion criteria prevent study participants from using anything other than the agent the trial is investigating. A major problem is that often the results of those clinical trials do not reflect clinical practice because very few people use the product in isolation. Our goal was to study people who say, ‘My eyes still bother me even though I am using various dry eye treatments. What else can I do?’ It is very rare in clinical practice to advise a patient to stop everything he or she is doing and use only omega-3.”
NOT ALL AGREE
The DREAM outcomes inspired a range of responses from other ophthalmologists and stakeholders in the DED arena interviewed by Bryn Mawr Communications. Some questioned the design of the study, with particular emphasis on its use of olive oil as a placebo; others described the study as well done, thorough, and appropriately mindful of real-world conditions.
Alice T. Epitropoulos, MD, an ocular surface disease expert at The Eye Center of Columbus, Ohio, and a clinical assistant professor at The Ohio State University Wexner Medical Center in Columbus, said she plans to continue recommending a reesterified omega-3 supplement to her patients with DED.
“A good quality reesterified omega-3 is becoming widely accepted as a primary therapy for dry eye patients,” Dr. Epitropoulos said. She is first author of a recently published paper that demonstrated benefits of reesterified omega-3 supplements in patients with DED in a multicenter, prospective, interventional, placebo-controlled, double-masked study.3 “Patients were excluded from our study if they were using topical cyclosporine, topical corticosteroids, and oral omega-3 fatty acids within 3 weeks of screening or any time during the study,” she explained. “Our results showed a statistically significant reduction in tear osmolarity—our primary endpoint—in the omega-3 group, at weeks 6 and 12, compared to control. We also saw a statistically significant improvement in TBUT, omega-3 index levels (indicating good absorption), along with a significant reduction in OSDI symptom scores and matrix metallopeptidase 9 positivity.” The study was funded by Physician Recommended Nutriceuticals (PRN).
Dr. Asbell pointed out that the DREAM researchers also analyzed the results for only the patients in DREAM who would have fulfilled the eligibility criteria for Dr. Epitropoulos’ study. “The combination of high osmolarity and mild meibomian gland disease [MGD] required for the Epitropoulos et al study was rare in DREAM,” she said. “Not all DREAM centers had the »TearLab osmometer, so only 375 of the 535 DREAM patients could be classified. Among these 375 patients, only 24 (6%) would have met the eligibility criteria, mostly because of the requirement of tear osmolarity of 312 mOsm/L or greater in at least one eye. Eligibility criteria also included mild MGD (moderate to severe MGD patients were excluded), and patients were excluded if they were using topical cyclosporine 0.05% (Restasis, Allergan), topical corticosteroids, nonsteroidal antiinflammatory drugs, glaucoma medications, or oral omega-3 fatty acids. With only 17 patients assigned to omega-3 and seven to placebo, no meaningful analysis could be performed.”
Laura M. Periman, MD, a Seattle-area private practice ophthalmologist and ocular surface disease expert, said she will also continue recommending omega-3 supplements to her patients with DED, although she said she thought the DREAM study was “well done,” and “appropriately mindful of more real-world conditions.”
Dr. Periman pointed out that, in situations in which study outcomes challenge the status quo, it is “tempting for clinicians to throw the baby out with the bathwater based on one study.” She added that it is important to keep in mind “that it is scientifically disingenuous to draw comparisons and conclusions between studies with completely different materials, methods, designs, and primary endpoint metrics.”
“I think one of the challenges presented by the results of a large study such as DREAM is that it is not easily distillable into sound bites, which is additive to the confusion regarding the actual paper and findings and even clinical trial design,” Dr. Periman said.
Cynthia Matossian, MD, FACS, medical director of Matossian Eye Associates, in New Jersey and Pennsylvania, said, “Omega-3s play a significant role as a foundation for my dry eye management.” She was a principal investigator in the Epitropoulos study of oral reesterified omega-3 supplementation,3 which she said showed that “omega-3s in the correct form and dose show statistical significance over placebo in known dry eye endpoints” as outlined in the Tear Film & Ocular Surface Society Dry Eye Workshop II,4 including tear osmolarity, TBUT, and corneal staining. She added that the DREAM outcomes will have no bearing on her prescribing habits. “My starter triad will continue to be preservative-free artificial tears, omega-3s in a reesterified triglyceride formulation, and a heated microwaveable mask from Bruder.”
THE OLIVE OIL PLACEBO
Dr. Asbell explained that the use of olive oil as the placebo did not dilute the strength of the DREAM outcomes for several reasons. First, she noted, 1 tsp of olive oil a day is less than what the average person might consume in his or her daily salad dressing, and the olive oil consumed daily in the popular Mediterranean diet is 12 times the amount used daily in the DREAM study (Figure 1). Second, the DREAM study used refined olive oil, which does not include all of the components of typical olive oil, such as polyphenols. Third, and perhaps most important, olive oil–related fatty acid blood level measurements, an objective metric, were essentially the same at baseline for the active group and the placebo group and did not change throughout the year of the study.
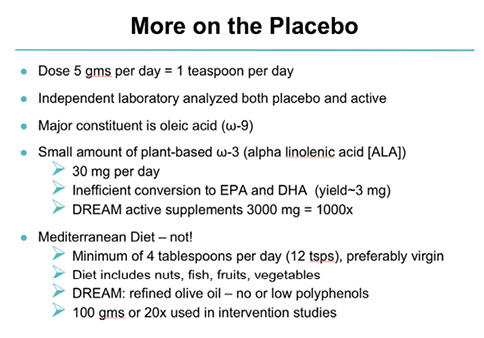
Figure 1. Each placebo dose contained 5 g of olive oil, equal to approximately 1 tsp.
“Oleic acid and alpha-linolenic acid were not very high at baseline, and they continued to be about the same at 6 and 12 months (Figures 2 and 3). There is no evidence that the olive oil—either by volume or by blood tests—was a significant factor in the results,” Dr. Asbell said. “If those two markers on red blood cells had increased over the year in one group and not the other, then I might also be thinking that there was a difference, but we did not see any difference at baseline and we did not see any difference over the year, and the levels we saw were not very high; they were standard in the American population.”
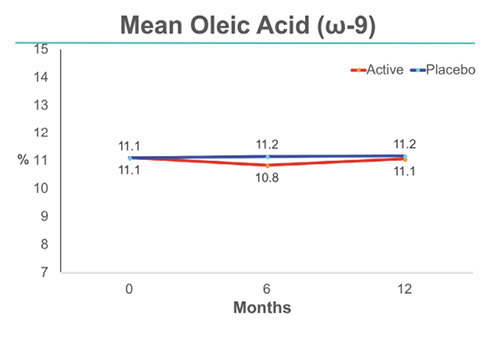
Figure 2. At 6 and 12 months, mean oleic acid was 5 to 6 times higher in the active group; there was no change in the placebo group.
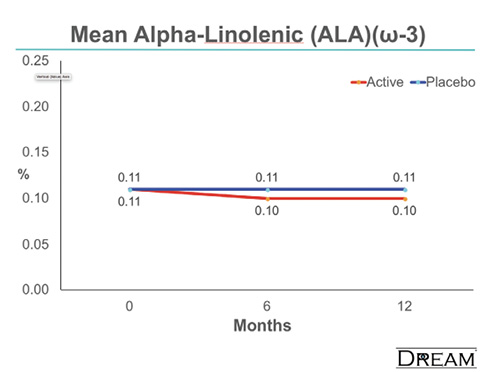
Figure 3. At 6 and 12 months, mean alpha-linolenic acid acid was 5 to 6 times higher in the active group; there was no change in the placebo group.
Dr. Asbell said the researchers would have liked to use water for the placebo, “but that was not an option. Gel caps have to be filled with an oil. Water cannot be used because it would seep out.”5
The DREAM study designers spent considerable time deciding what the placebo should be, Dr. Asbell said. Artemis P. Simopoulos, MD, FACN, was among the many nutritional experts with whom they consulted. “It was brought to our attention by Dr. Simopoulos that omega-3 trials, including those for cardiovascular disease, asthma, rheumatoid arthritis, and other conditions, often used olive oil as a placebo. So it was not an unusual choice for us to use olive oil as well,” she said. Dr. Simopoulos was a founding member of the International Society for the Study of Fatty Acids and Lipids and is the founder and president of the Center for Genetics, Nutrition and Health, a nonprofit educational organization in Washington, DC.
Dr. Epitropoulos noted that, although the amount of olive oil used in the placebo may have been less than that in the Mediterranean diet, it still has active antiinflammatory properties with potential for DED healing. “If anything, the DREAM study showed that olive oil might be another alternative to fish oil,” she said. “Both arms improved, so that does not mean omega-3s do not work—it means both products worked. The negative results were overstated because they were not reported in the context of omega-3s as an add-on therapy. Given that many of the trial participants were already using other treatments—including omega-3s—upon recruitment and continued to use them throughout the study, this was not a monotherapy study of omega-3 alone. Furthermore, the use of additional dry eye therapies was not controlled. Participants in both arms, active supplement and olive oil, were permitted to increase, decrease, or otherwise change the number and types of concurrent therapies utilized during the study. In fact, 75% of participants in the active group and 78% in the placebo group reported a change in their treatment regime over the course of the study.”
Anat Galor, MD, MSPH, of the Bascom Palmer Eye Institute at the University of Miami Miller School of Medicine in Florida, said that she typically mentions omega-3s to her patients who have DED as part of a multimodal approach, but she will now also update her patients on the recent findings of the DREAM study. “The amount of olive oil used as placebo was small compared to a Mediterranean diet,” she said. “Also, regression to the mean is commonly seen in trials, so I am not surprised both groups got a little better. Overall, I remain positive about the trial design, even though it was not perfect, as well as about the validity of findings, even though there can be other interpretations.”
Dr. Periman noted that, although she would have liked to see a no-treatment observation group in the DREAM study, she agrees that “fish oil did not outperform olive oil; they both appeared to be of benefit.” She pointed out that the metrics used may be more of an issue than study design or placebo choice. “I think that the DREAM study, as well as 14 failures at FDA approval for new DED therapeutics, highlights a larger problem with dry eye trials. We do not have outcome metrics with good sensitivity and specificity. We do not have clear delineations between different dry eye subtypes. Maybe the ocular surface disease population is actually 10 to 20 diseases instead of two to three,” she said. “Traditional metrics such as staining and Schirmer and [Standardized Patient Evaluation of Eye Dryness] scores have low sensitivity and specificity. This creates a challenge in discerning signal from noise. We need more accurate methods for studying disease activity on immunologic and neurologic levels. So if data show no effect, it could be that there truly is no effect, or it could mean that the study population and disease state was not homogeneous, or it could mean that the wrong endpoint was studied, or it could mean that we need a different measuring stick.”
SUBGROUP ANALYSES
John D. Sheppard, MD, MMSC, FACS, of Virginia Eye Consultants and the department of ophthalmology at Eastern Virginia Medical School in Norfolk, said, “I’m delighted with the discipline in the DREAM study, looking at a very closely purified and esterified omega-3 essential fatty acid source for patients with dry eye disease. The fascinating outcome was that there was no differential effect upon signs and symptoms of dry eye disease. However, subpopulation segmented analyses of different types of patients; their nutritional status; their age; their absorption status; and many other factors in the diet, lifestyle, and underlying disease may reveal different subsets of patients who do indeed respond.”
Dr. Asbell pointed out that the DREAM study looked at four prespecified subgroups. There was no difference between omega-3 and placebo in patients with high or low blood levels of EPA and DHA at baseline, with severe symptoms or mild symptoms, with severe signs or mild signs, or with or without inflammation as measured by human leukocyte antigen-DR expression. Exploratory analyses were performed on 18 additional features, and none found significant differences. She questioned the value of analyzing even more subgroups after the fact. “If you look long enough, eventually you will find some significance, but most statisticians would say that doing subgroup analyses after the fact, and doing them over and over until you find that one group that is statistically significant, is likely to lead to a false conclusion,” she said.
Dr. Sheppard noted that the DREAM study’s results “are in direct contradistinction to our study using a combination of omega-3s and gamma-linolenic acid [GLA] in the form of black currant seed oil,6 as well as the large, multicenter, prospective, placebo-controlled study by the Epitropoulos group looking at another type of omega-3 supplement.”3 He noted, however, that both of those studies were industry sponsored. “So perhaps a double-blinded study with a GLA-containing commercial product, without commercial sponsorship, corroborating the DREAM study analysis may give us results that are more consistent with some of the populations that we see as surgeons,” he proposed. “GLA alone is an effective treatment for contact lens– and Sjögren syndrome–associated dry eye.”7,8
He continued, “The equivalent therapeutic response in both DREAM groups logically arouses suspicions that even low doses of the refined, very low phenolic content olive oil control may have a significant therapeutic effect, particularly in real-life scenarios where overall dietary intake quality is often suboptimal. Oleic acid, the predominant fatty acid in olive oil, offsets the inflammatory effect of a high fatty acid diet and may counteract arachidonic acid.”9,10
REAL-WORLD STUDY, REAL-WORLD IMPACT
Dr. Matossian noted that there has been substantial coverage of the DREAM study results in the mainstream media with headlines such as, “Fish Oil Supplements Ineffective Against Dry Eye,”11 and that this is a concern because it may influence patients.
“I’m hopeful that the patients will consult their doctors before making a change to their dry eye treatment, should it include omega-3s,” she said. “The study was loosely controlled, and I don’t believe that the results were strong enough to provide evidence to the eye care industry—including patients—to stop taking omega-3s.”

1. Dry Eye Assessment and Management Study Research Group; Asbell PA, Maguire MG, Pistilli M, et al. n-3 fatty acid supplementation for the treatment of dry eye disease. N Engl J Med. 2018;378(18):1681-1690.
2. Dry Eye Syndrome PPP – 2013. American Academy of Ophthalmology. www.aao.org/preferred-practice-pattern/dry-eye-syndrome-ppp–2013. Accessed May 22, 2018.
3. Epitropoulos AT, Donnenfeld ED, Shah ZA, et al. Effect of oral re-esterified omega-3 nutritional supplementation on dry eyes. Cornea. 2016;35(9):1185-1191.
4. Dry eye redefined: TFOS DEWS II Report. Tear Film & Ocular Surface Society. www.tfosdewsreport.org/. Accessed May 22, 2018.
5. Neeley CK. How to dissolve gel caps. July 27, 2017. https://healthfully.com/dissolve-gel-caps-8241095.html. Accessed May 22, 2018.
6. Sheppard JD Jr, Singh R, McClellan AJ, et al. Long-term supplementation with n-6 and n-3 PUFAs improves moderate-to-severe keratoconjunctivitis sicca: a randomized double-blind clinical trial. Cornea. 2013;32(10):1297-1304.
7. Kokke KH, Morris JA, Lawrenson JG. Oral omega-6 fatty acid treatment in contact lens associated dry eye. Cont Lens Anterior Eye.2008;31(3):141-146.
8. Aragona P, Bucolo C, Spinella R, et al. Systemic omega-3 essential fatty acid treatment and PGE1 tear content in Sjogren’s syndrome patients. Invest Ophthalmol Vis Sci. 2005;46:4474-4479.
9. Basu A, Devaraj S, Jialat I. Dietary factors that promote or retard inflammation. Arterioscler Thromb Vasc Biol. 2006;26:995-1001.
10. Hostmark A, Haug A. Percentages of oleic acid and arachidonic acid are inversely related in phospholipids of human sera. Lipids Health Dis. 2013;12:106.
11. Emery G. Fish oil supplements ineffective against dry eye. Reuters. April 13, 2018. www.reuters.com/article/us-health-dryeye-fishoil-trial/fish-oil-supplements-ineffective-against-dry-eye-idUSKBN1HK2JT. Accessed May 22, 2018.