



The advanced dry eye clinic in which I work is an integral part of our practice’s collaborative care clinic. It is a specialized clinic where optometrists can send patients who have exhausted all other options.
Recent estimates are that 16 million Americans have been diagnosed with dry eye disease (DED), but DED remains an underdiagnosed condition. As many as 30 million Americans may actually have the condition.1,2 Fortunately, the eye care professions have made significant advances in understanding the etiology and pathogenesis of DED, which in turn has led to more accurate diagnoses and new treatment options for this multifactorial disease.3
Two patients who recently presented to our dry eye clinic may be of interest to CollaborativeEYE readers.
CASE No. 1: PERSISTENT EPITHELIAL DEFECTS
A 68-year-old white woman was referred to our clinic for a DED evaluation. She had been experiencing burning and stinging eyes and foreign body sensation over the past few years but had recently also noted fluctuating vision. She had cataract surgery 2 years before her visit: A »Tecnis multifocal IOL (Johnson & Johnson Vision) was placed in each eye. Her optometrist had treated her previous DED symptoms with cyclosporine ophthalmic emulsion 0.05% (»Restasis, Allergan), temporary punctal plugs, a month-long steroid taper, and multiple over-the-counter tears—all of which resulted in little relief.
Upon examination, the patient’s VA was 20/25 at distance and J3 at near. Her tear breakup time (TBUT) was 3 seconds in both eyes, which correlated with telangiectatic lid margins. Her corneas had 1 to 2+ punctate epithelial erosions (OS > OD).
Initiating Therapy
The patient was started on lifitegrast ophthalmic solution 5% (»Xiidra, Shire) and received cryopreserved amniotic membrane (»Prokera, Bio-Tissue) on her left eye. At 1 week, her VA was 20/20 at distance and J1 at near. We performed a series of four intense pulsed light (IPL; »M22, Lumenis) treatments 1 month later. After her fourth treatment, the patient reported a significant improvement in the burning and foreign body sensation symptoms and significantly less fluctuating vision.
A recent review of data from the Centers for Medicare and Medicaid Services found that only 1% of optometrists in the United States placed an amniotic membrane in the past year.4 We expect this number to increase in light of a study by Thomas John, MD, that showed improvement in symptoms, pain, TBUT, and corneal staining, as well as increased corneal nerve density and sensitivity, in DED patients after placement of cryopreserved amniotic membrane.5
In this patient, amniotic membrane was used to regenerate the ocular surface, and IPL addressed the root issue of meibomian gland dysfunction. In IPL, high intensity noncoherent light is used to coagulate telangiectatic vessels seen in meibomian gland dysfunction and ocular rosacea. Reduction of inflammation from these leaky blood vessels reduces the level of cytokines in the tear film, and patients experience improved TBUT and decreased symptoms.6-8
CASE No. 2: TREATING THE OCULAR SURFACE BEFORE CATARACT SURGERY
A 68-year-old woman was referred to our clinic for a combined cataract/DED evaluation by her optometrist. The patient was hoping to reduce her dependence on glasses after cataract surgery. Her tear osmolarity test indicated 293 mOsm/L OD and 303 mOsm/L OS, and noninvasive TBUT was 4 seconds in each eye. Examination showed 50% gland atrophy and migration of cosmetic products into the tear film, and topography showed inferior steepening suggestive of evaporative DED.9
Initiating Therapy
The patient was started on cyclosporine twice a day in both eyes and loteprednol etabonate ophthalmic suspension 0.5% (Lotemax, Bausch + Lomb) twice a day in both eyes.
The patient noted improvement in visual fluctuation after 1 month, but her topography still showed inferior steepening. She underwent vectored thermal pulsation (»LipiFlow, Johnson & Johnson Vision). Topography had improved 1 month later (Figure).
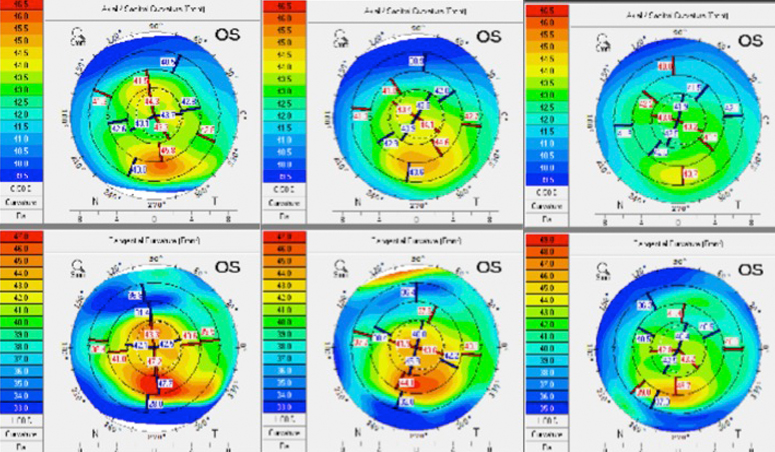
Figure. Initial topography in patient with DED consistent with keratoconus-like steepening of interior cornea (left), which improved after 1 month of topical treatments (middle). After vectored thermal pulsation, a significant improvement in signs and symptoms was observed (right).
The patient subsequently underwent cataract surgery in both eyes. Her postoperative VA is 20/20 at distance, J1 at intermediate, and J1 at near. She was referred back to her optometrist for continued care.
Tear osmolarity, noninvasive TBUT, and topography can aid in making an accurate diagnosis of DED during a cataract evaluation.9-11 Treating the tear film aggressively before surgery is mandatory, especially in premium IOL patients. We favor a single vectored thermal pulsation treatment over low dose doxycycline or warm compresses to restore the homeostasis of the tear film as quickly as possible before cataract surgery.12
SHINING EXAMPLES OF COLLABORATION
These two cases illustrate how community optometrists and surgical practices can work together to make sure every patient has a high-quality experience—and that each discipline is given its best chance to shine.

- Nichols KK, Foulks GN, Bron AJ, et al. The international workshop on meibomian gland dysfunction: executive summary. Invest Ophthalmol Vis Sci. 2011;52(4):1922-1929.
- Farrand KF, Fridman M, Stillman IO, et al. Prevalence of diagnosed dry eye disease in the United States among adults aged 18 years and older. Am J Ophthalmol. 2017;182:90-98.
- Craig JP, Nelson JD, Azar DT, et al. TFOS DEWS II report executive summary. Ocul Surf. 2017:15(4):802-812.
- ODWire.org. Shocker: Only 1% of ODs Use Amniotic Membranes. Published June 27, 2018. https://www.odwire.org/shocker-1-ods-use-amniotic-membranes. Accessed July 10, 2018.
- John T, Tighe S, Sheha H, et al. Corneal nerve regeneration after self-retained cryopreserved amniotic membrane in dry eye disease. J Ophthalmol. 2017;2017:6404918.
- Vegunta S, Patel D, Shen JF. Combination therapy of intense pulsed light therapy and meibomian gland expression (IPL/MGX) can improve dry eye symptoms and meibomian gland function in patients with refractory dry eye: a retrospective analysis. Cornea. 2016;35(3):318-322.
- Dell SJ, Gaster RN, Barbarino SC, Cunningham DN. Prospective evaluation of intense pulsed light and meibomian gland expression efficacy on relieving signs and symptoms of dry eye disease due to meibomian gland dysfunction. Clin Ophthalmol. 2017;11:817-827.
- Liu R, Rong B, Tu P, et al. Analysis of cytokine levels in tears and clinical correlations after intense pulsed light treating meibomian gland dysfunction. Am J Ophthalmol. 2017;183:81-90.
- De Paiva CS, Harris LD, Pflugfelder SC. Keratoconus-like topographic changes in keratoconjunctivitis sicca. Cornea. 2003;22(1):22-24.
- Wolffsohn JS, Arita R, Chalmers R, et al. TFOS DEWS II diagnostic methodology report. Ocul Surf. 2017;15(3):539-574.
- Trattler WB, Majmudar PA, Donnenfeld ED, et al. The prospective health assessment of cataract patients’ ocular surface (PHACO) study: the effect of dry eye. Clin Ophthalmol. 2017;11:1423-1430.
- Hagen KB, Bedi R, Blackie CA, Christenson-Akagi KJ. Comparison of a single-dose vectored thermal pulsation procedure with a 3-month course of daily oral doxycycline for moderate-to-severe meibomian gland dysfunction. Clin Ophthalmol. 2018;12:161-168.

