


Patients with keratoconus can experience disease progression at any age, but it tends to be more rapidly aggressive in younger patients than those who are middle-aged or older. One of the greatest challenges occurs when children or adolescents present with keratoconus in one or both eyes. Patients and their families want to know how urgent corneal collagen cross-linking (CXL) is—for example, can the procedure wait a few months for a school holiday or summer vacation, or should it be performed in the next few weeks? Eye care providers should take this opportunity to educate patients and their parents about the realities of keratoconus.
CASE EXAMPLE
A 10-year-old boy with keratoconus presented for a consultation in January 2014 (Figure 1). The maximum corneal curvature (Kmax) in his right eye was 58.70 D, and the corneal thickness was 521 µm. The family asked if it would be okay to schedule CXL for spring break and, after a lengthy discussion, decided to wait until April for the procedure.
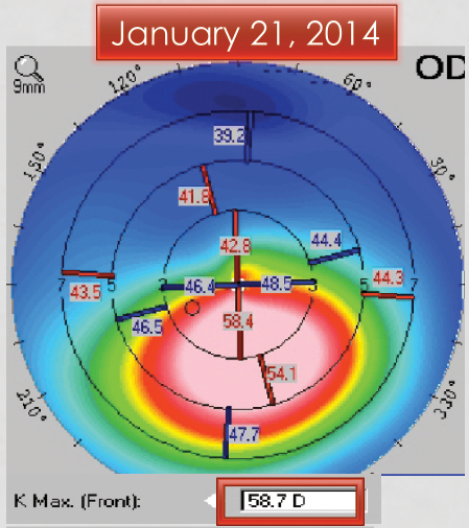
Figure 1. Initial presentation. Significant inferior corneal steepening is consistent with keratoconus.
Unfortunately, when the patient returned 3 months later, the keratoconus had progressed significantly. The Kmax had steepened to 63.00 D, and the cornea had thinned to 506 µm (Figure 2). The patient had also lost 1 line of BCVA. He underwent CXL in April 2014, and the procedure stabilized both eyes.
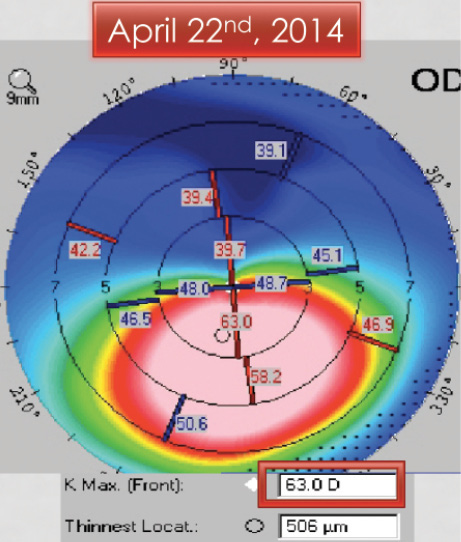
Figure 2. Three months later, the patient returned for CXL. The keratoconus progressed significantly, with an increase in Kmax to 63.00 D and thinning of the cornea.
LESSONS LEARNED
As this case demonstrates, it is important for clinicians to be aware that keratoconus can progress rapidly during childhood and adolescence. Although the frequency of follow-up visits with repeat corneal mapping to identify disease progression for adults can range from every 6 to 12 months, children and adolescents may require shorter intervals. On examination, the two tests that are most helpful in determining the stability or progression of keratoconus are refraction with BCVA and corneal imaging (topography/tomography).
Once keratoconus has been diagnosed, a discussion of the risks and benefits can help the patient and his or her family understand how CXL can have a significant impact on preventing the condition from worsening. CXL halts the progression of keratoconus and improves corneal shape. Many patients who have undergone the procedure can experience some improvement in quality of vision and BCVA.
CONCLUSION
Although CXL is not considered an emergency procedure, it is important to monitor young patients and adolescents with keratoconus closely. Disease progression can occur rapidly in this population. CXL has a long history of helping patients with keratoconus, and clinicians’ understanding of the procedure’s importance in patients with progressive disease is improving.